양성급성소아기근육염 또는 횡문근융해증으로 응급실을 방문한 소아환자의 임상적 특징과 신대체요법 적용
Abstract
Purpose
This study was performed to analyze clinical features and use of renal replacement therapy (RRT) for children who visit the pediatric emergency department with benign acute childhood myositis (BACM) or rhabdomyolysis.
Methods
We retrospectively reviewed medical records of 289 children who visited the emergency department with BACM or rhabdomyolysis from January 2013 through December 2022. Clinical features, laboratory and microbiological findings, and outcomes were compared between children with the 2 diagnoses. Subsequently, multivariable logistic regressions were performed to identify factors associated with applying RRT.
Results
Of the 289 children, a total of 212 were analyzed, including 93 with BACM and 119 with rhabdomyolysis. Influenza (70 of the 145 children [48.3%]) was the most common cause, followed by exercise (36 of 212 [17.0%]). Compared with the children with BACM, those with rhabdomyolysis showed significantly higher frequencies of being boys and hematuria, and higher concentrations of hemoglobin, creatinine, creatine kinase, and myoglobin. Continuous venovenous hemofiltration, a modality of RRT, was applied to 8 children (6.7%) with rhabdomyolysis, of whom 1 died. Creatine kinase was independently associated with the application of RRT (adjusted odds ratio, 1.06; 95% confidence interval, 1.00-1.12; P = 0.036).
Conclusion
Rhabdomyolysis in children who require RRT may be associated with a higher concentration of creatine kinase.
Key Words: Child; Myositis; Renal Replacement Therapy; Rhabdomyolysis; Risk Factors
서론
양성급성소아기근육염(benign acute childhood myositis, BACM)과 횡문근융해증은 공통으로 바이러스 감염, 특히 인플루엔자 감염 이후 다리의 뼈대 근육 통증 또는 보행장애를 유발한다. 하지만 신체검사에서 두 질환 모두 유사하게 이환된 뼈대 근육의 압통은 동반하지만, 관절의 부종, 발적, 운동범위 제한, 깊은 힘줄반사 저하는 동반하지 않아 서로 감별하기 어렵다( 1- 5). BACM은 주로 열을 동반한 감염병이 선행(先行)하는데, 명확한 치료법 없이 지지요법을 시행하고, 합병증 없이 일주일 내외에 호전된다( 1, 2). 횡문근융해증도 대개 바이러스 감염이 원인이지만, 과도한 운동, 약, 대사질환 등 더 다양한 원인을 가지며, 혈청 크레아틴인산화효소가 1,000 U/L 또는 정상 상한선의 5배 이상으로 증가한다( 3, 4). 횡문근융해증 환자의 5.0%-35.9%에서 다양하게 급성콩팥손상을 유발할 수 있다고 보고됐지만, 관련된 한국 소아 보고는 적었다( 6- 9). 본 저자는 비슷한 증상으로 응급실을 방문하지만, 경과가 서로 다를 수 있는 BACM 및 횡문근융해증의 임상양상을 비교하고, 두 질환으로 인한 급성콩팥손상에 신대체요법을 적용하는 것과 연관된 위험인자를 확인하고자 본 연구를 수행했다.
대상과 방법
1. 대상
2013년 1월-2022년 12월에 단일 3차 대학병원 응급실을 방문한 18세 이하 환자 중, 퇴원 진단에 국제질병분류 10판에 따른 근육염 코드(M60) 또는 횡문근융해증 코드(M62)가 기재된 환자를 추출하여, 의무기록을 분석했다. 두 코드를 모두 가진 환자는 11명이었고, 응급실에서 시행한 검사에서 크레아틴인산화효소가 1,000 U/L 미만인 경우를 BACM으로, 그 이상인 경우를 횡문근융해증으로 각각 분류했다. 제외기준은 대사질환, 외상, 세균관절염, 근디스트로피, 이송이었다. 본 연구는 본원 임상연구심의위원회로부터 연구 프로토콜을 승인받았으며, 후향적 연구 특성상 연구대상자 동의는 면제받았다(IRB no. 2023-1431).
2. 방법
표준 증례보고 양식을 이용하여, 모든 변수는 응급실에서 시행한 검사 결과에서 수집했다. 구체적으로, 나이 및 나이대(영유아기[0-2세], 학령전기[3-5세], 학령기[6-10세], 청소년기[11-18세]), 성별, 체온, 추정 원인, 응급진료 결과(전체 및 중환자실 입원, 신대체요법, 병원내 사망), 합병증 발생, 백혈구, 혈색소, 혈소판, C반응단백질, 혈액요소질소, 크레아티닌, 크레아틴인산화효소, 근색소, 혈뇨, 단백뇨, 바이러스 중합효소사슬반응(BD MAX; Becton, Dickinson and Company) 결과를 수집했다. 치료 경과는 BACM 및 횡문근융해증으로, 그리고 횡문근융해증 환자는 지지요법 및 신대체요법 적용 환자로 각각 나누어 분석했다.
3. 통계
통계 분석에 IBM SPSS Statistics for Windows, ver. 21 (IBM Corp.)을 사용했고, P < 0.05를 통계적 유의성으로 정의했다. 연속형 변수는 평균 및 표준편차 또는 중앙값 및 사분위수 범위로, 범주형 변수는 수 및 백분율로 각각 기술했다. 연속형 변수는 Student t-test 또는 Mann-Whitney U-test를, 범주형 변수는 chi-square test 또는 Fisher exact test를 각각 이용하여 분석했다. 여기에서 유의한 변수 및 단변수 로지스틱 회귀분석에서 유의한 변수를 독립변수로, 신대체요법 적용을 종속변수로 정의하여 다변수 로지스틱 회귀분석을 시행했다.
결과
연구기간에 BACM 또는 횡문근융해증으로 진단된 총 212명의 환자를 분석했고, 이 중 BACM은 93명, 횡문근융해증은 119명이었다( Fig. 1). Table 1에 BACM 군과 횡문근융해증 군의 임상적 특성을 비교했다. 횡문근융해증 군에서 나이의 중앙값이 크고, 청소년기 비율이 높은 경향을 보였으며(P = 0.110), 남자 비율이 높았다. BACM 및 횡문근융해증의 추정 원인을 Fig. 2에 요약했다. 구체적으로, BACM은 감염이 가장 많았고(80명[86.0%]; 영유아기 5명, 학령전기 32명, 학령기 32명, 청소년기 11명), 운동이 뒤를 이었다(9명[9.7%]; 학령기 5명, 청소년기 4명). 횡문근융해증에서도 감염이 가장 많았고(90명[75.6%]; 영유아기 4명, 학령전기 36명, 학령기 38명, 청소년기 12명), 운동이 뒤를 이었다(27명[22.7%]; 학령전기 1명, 학령기 1명, 청소년기 25명). 하지만 청소년기에서 BACM 및 횡문근융해증의 가장 흔한 원인은 운동으로, 다른 나이대보다 흔했다(53명 중 29명[54.7%], P < 0.001). 감염원으로는 바이러스, 특히 인플루엔자(145명 중 70명[48.3%])가 가장 흔했다( Fig 3, Appendix 1 [ https://doi.org/10.22470/pemj.2023.00892]). 급성콩팥손상으로 신대체요법을 적용한 환자는 8명(6.7%)으로 모두 횡문근융해증 환자였고, 지속적 정정맥 혈액투석여과(continuous venovenous hemofiltration)를 경험했다. 이 중 1명은 다기관부전으로 사망했다. 혈액검사는 횡문근융해증에서 혈색소, 크레아티닌, 크레아틴인산화효소, 근색소 농도가 높고, 혈뇨가 흔했다( Table 1). 횡문근융해증에서 지지요법을 시행한 군과 지속적 정정맥 혈액투석여과를 시행한 군을 분석한 결과, 후자에서 백혈구, 혈색소, 혈액요소질소, 크레아티닌, 크레아틴인산화효소, 근색소 농도가 높고, 혈뇨 및 단백뇨가 흔했다( Table 2). 다변수 로지스틱 회귀분석 결과, 크레아틴인산화효소 농도가 높을 때 지속적 정정맥 혈액투석여과의 위험도가 증가하는 것을 확인했다(보정 교차비, 1.06; 95% 신뢰구간, 1.00-1.12; P = 0.036) ( Table 3).
고찰
본 연구에서 BACM과 비교하여 횡문근융해증이 남자 또는 나이가 많은 환자에서 발생하는 경향을 보였다. 두 질환이 청소년기 이전 시기에는 주로 감염에 기인하는 것과 달리, 청소년기 환자는 격렬한 운동으로 인해 크레아틴인산화효소가 현저히 상승하는 것으로 추론한다( Fig. 2). 두 질환 모두 명확한 치료 지침이 없어( 2, 3), 해열진통제와 함께 등장액(예: 0.9% 식염수)을 20 mL/kg로 투여 후 유지 용량의 2배로 투여하며 소변량을 유지하는 것이 중요하다( 3, 8). BACM에서 급성콩팥손상은 발생하지 않았고, 횡문근융해증에서는 8명(6.7%)이 신대체요법을 경험했는데, 이는 이전에 보고된 3.7%-7.8%와 비슷하다( 4, 6, 8). 급성콩팥손상의 위험인자로 이전 연구에서 초기 크레아틴인산화효소, 근색소, 단백뇨 등을 보고했다( 7- 11). 본 연구에서 크레아틴인산화효소 및 근색소 외에 혈색소, 크레아티닌이 횡문근융해증에서 유의하게 증가했으며 단백뇨와 혈뇨에서 유의한 차이를 보였다. 감염원 중 인플루엔자가 가장 흔했는데, 그 빈도(48.3%)는 이전 연구의 인플루엔자 빈도(37%-78%)와 비슷하다( 4, 8, 12). 본 연구에서 사람 보카바이러스(human bocavirus) 및 아데노바이러스 연관 횡문근융해증 환자가 각 1명 있었는데, 저자가 알기로는 이들 바이러스는 이전에 보고되지 않았다. 뎅기바이러스 연관 BACM 및 횡문근융해증 환자는 각 1명 및 2명이었고, 인도와 동남아시아 등지에서는 자주 보고됐지만( 13) 한국에서는 1례만 보고됐다( 14). BACM과 횡문근융해증 사이에 유의한 차이를 보인 남자, 혈색소, 크레아티닌, 근색소, 혈뇨는 회귀분석에서는 유의하지 않았다. 횡문근융해증에서 지지요법을 시행한 군과 지속적 정정맥 혈액투석여과를 시행한 군 비교에서 유의한 차이를 보인 변수로 시행한 회귀분석에서는 크레아틴인산화효소만이 지속적 정정맥 혈액투석여과 적용과 독립적 연관을 보였다( Table 3). 본 연구와 달리, 중환자실에 입원하여 신대체요법을 적용한 환자를 분석한 연구에서는 크레아틴인산화효소와 연관되지 않음을 보고했다( 15). 횡문근융해증에서 급성콩팥손상의 위험인자를 확인한 이전 연구와 달리, 본 연구는 신대체요법을 적용한 군의 위험인자를 분석했다는 의의가 있다. 대부분 연구에서 신대체요법을 시행한 표본의 크기가 작아 위험인자를 파악하기에 어려웠다( 8, 15). 미국 의료보험 데이터베이스를 기반으로 한 대규모 연구에서 기본 역학 자료만 분석한 결과, 입원 기간이 길거나 만성 질환을 가진 경우 신대체요법 적용이 증가했다고 보고했다( 7). Harmer 등( 4)은 10년간 단일 기관 연구에서 검사 내용에 관한 자세한 설명 없이, 소변검사에 이상이 있는 경우 신대체요법을 더 자주 시행했다고 보고했다. 본 연구의 제한점은 다음과 같다. 첫째, 후향적 단일기관 연구로, 모집단과 비교하여 다소 치우친 환자군이 포함됐을 수 있다. 둘째, 연구기간에 코로나바이러스병-19 범유행 기간이 포함되어, 기존의 바이러스 역학과 다를 수 있다. 하지만 10년간 비교적 많은 수의 환자를 분석했으므로, 이러한 제한점이 어느 정도 보완됐을 것으로 생각한다.
본 연구는 BACM 및 횡문근융해증의 임상적 특징 및 신대체요법을 적용한 환자와 지지요법을 받은 환자를 비교한 연구로, 횡문근융해증에서 남자, 청소년기, 혈뇨의 비율, 혈색소, 크레아티닌, 크레아틴인산화효소, 근색소 농도가 높게 나타났다. 특히, 횡문근융해증에서 크레아틴인산화효소 농도가 높을 때 신대체요법을 적용할 가능성이 증가하는 것을 확인했다.
Data availability
All data presented in this manuscript is available from the corresponding author upon reasonable request.
Fig. 1.
Enrollment of the study population. BACM: benign acute childhood myositis, ED: emergency department. 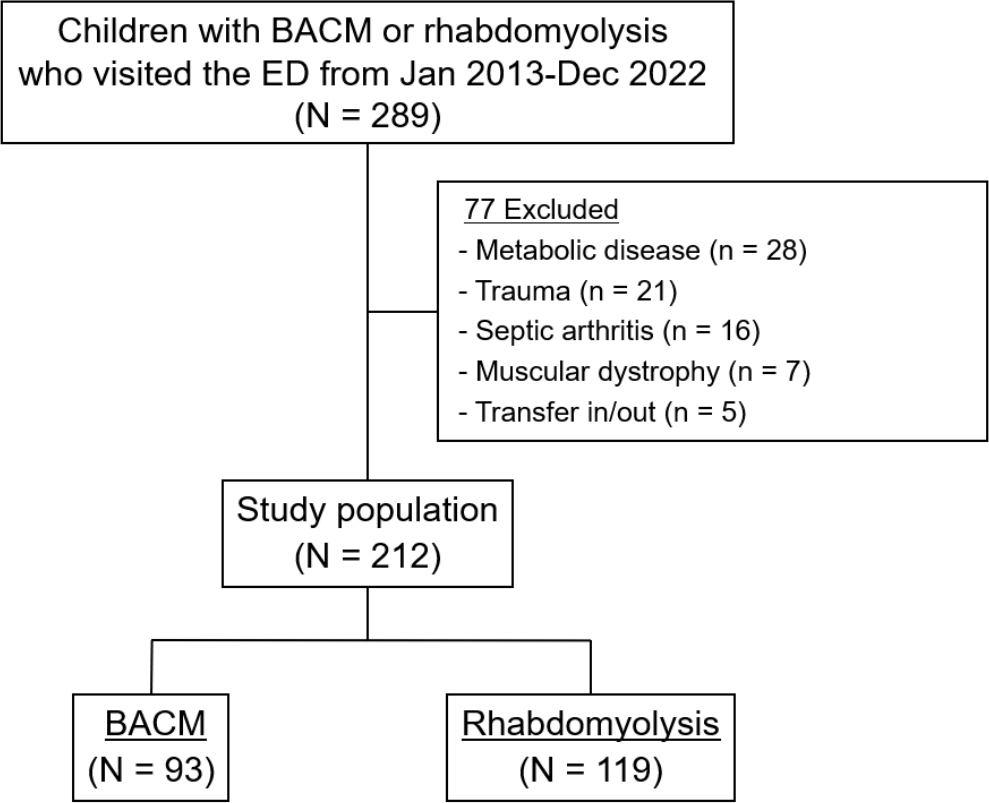
Fig. 2.
Causes of benign acute childhood myositis and rhabdomyolysis by the age groups. Open, gray shaded, and black shaded bars indicate infection, exercise, and unknown etiology, respectively. 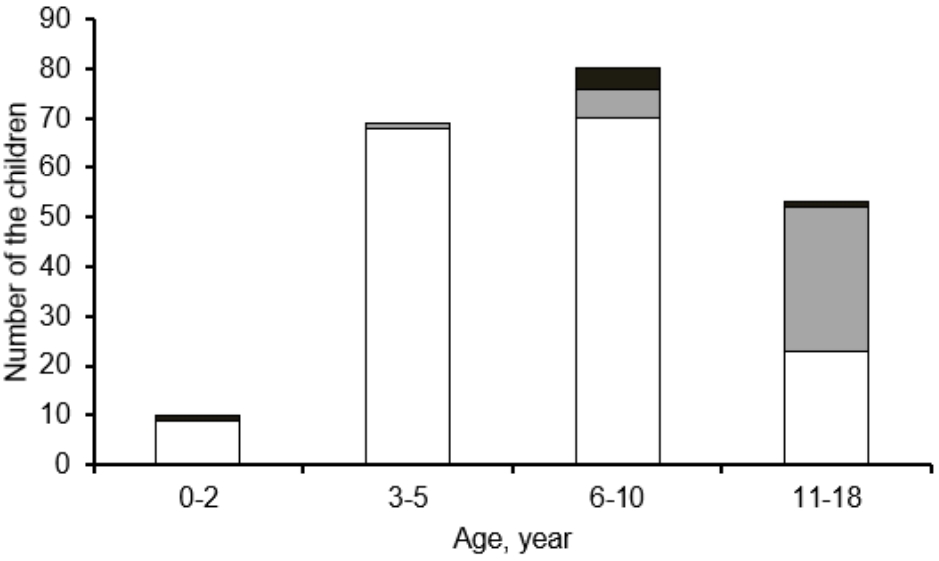
Fig. 3.
Causing organism of benign acute childhood myositis (open bars) and rhabdomyolysis (shaded bars). COVID-19: coronavirus disease 2019. 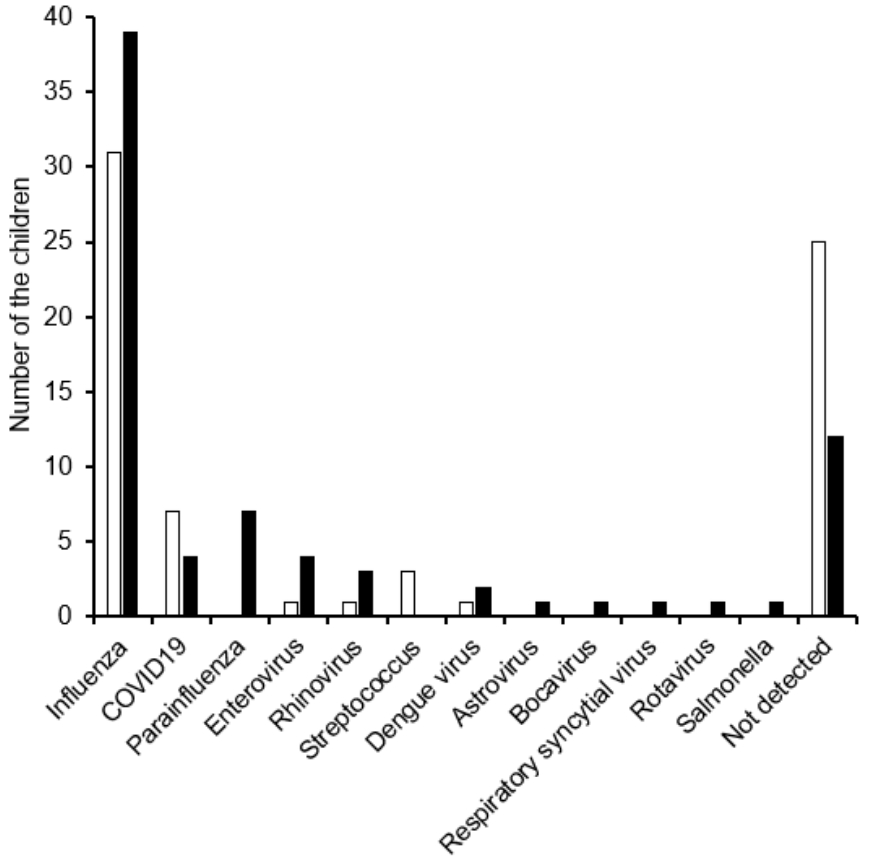
Table 1.
Comparison between the children with benign acute childhood myositis and those with rhabdomyolysis
|
Characteristic |
Total (N = 212) |
Benign acute childhood myositis (N = 93) |
Rhabdomyolysis (N = 119) |
P value |
|
Age, y |
6 (5-11) |
6 (4-9) |
7 (5-13) |
0.004 |
|
Age group, y |
|
|
|
0.11 |
|
0-2 |
10 (4.7)*
|
6 (6.5) |
4 (3.4)*
|
|
|
3-5 |
69 (32.5)*
|
32 (34.4) |
37 (31.1)*
|
|
|
6-10 |
80 (37.7)*
|
39 (41.9) |
41 (34.5)*
|
|
|
11-18 |
53 (25.0)*
|
16 (17.2) |
37 (31.1)*
|
|
|
Boys |
144 (67.9) |
51 (54.8) |
93 (78.2) |
< 0.001 |
|
Temp, ℃ |
37.3 ± 0.8 |
37.3 ± 0.8 |
37.3 ± 0.8 |
0.593 |
|
Laboratory data |
|
|
|
|
|
White blood cells, ×103/mm3
|
6.6 ± 3.9 |
6.6 ± 3.7 |
6.6 ± 4.1 |
0.899 |
|
Hemoglobin, g/dL |
13.1 ±1.1 |
12.8 ±1.1 |
13.1 ±1.5 |
< 0.001 |
|
Platelets, ×103/mm3
|
225.4 ± 80.6 |
235.5 ± 84.6 |
217.5 ± 76.8 |
0.106 |
|
C-reactive protein, mg/dL |
0.7 ± 1.4 |
0.7 ± 1.2 |
0.7 ± 1.6 |
0.756 |
|
Blood urea nitrogen , mg/dL |
12.4 ± 14.1 |
10.3 ± 3.0 |
14.1 ± 18.5 |
0.054 |
|
Creatinine, mg/dL |
0.9 ± 4.2 |
0.5 ± 0.1 |
0.8 ± 1.2 |
0.015 |
|
Creatine kinase, IU/L |
5,243.8 ± 5,872.6 |
486.8 ± 228.5 |
8,961.4 ± 2,046.2 |
< 0.001 |
|
Myoglobin, ng/mL |
1,097.8 ± 293.6 |
229.1 ± 360.7 |
1,776.6 ± 5,144.5 |
0.004 |
|
Hematuria |
44 (20.8) |
9 (9.7) |
35 (29.4) |
< 0.001 |
|
Proteinuria |
41 (19.3) |
13 (14.0) |
28 (23.5) |
0.081 |
|
Emergency department outcomes |
|
|
|
|
Hospitalization |
140 (66.0) |
22 (23.7) |
118 (99.2) |
< 0.001 |
|
Intensive care unit |
12 (5.7) |
1 (1.1) |
11 (9.2) |
0.014 |
|
Continuous venovenous hemofiltration |
8 (3.8) |
0 (0) |
8 (6.7) |
0.011 |
|
In-hospital mortality |
1 (0.5) |
0 (0) |
1 (0.8) |
> 0.999 |
Table 2.
Comparison of the children with rhabdomyolysis who underwent supportive care and continuous venovenous hemofiltration (N = 119)
|
Characteristic |
Supportive therapy (N = 111) |
continuous venovenous hemofiltration (N = 8) |
P value |
|
Temp, ℃ |
37.3 ± 0.8 |
37.6 ± 0.8 |
0.973 |
|
Age, y |
8.5 ± 5.0 |
10.5 ± 6.4 |
0.295 |
|
Exercise |
24 (20.3) |
3 (37.5) |
0.31 |
|
Laboratory data |
|
|
|
|
White blood cells, ×103/mm3
|
6.3 ± 3.9 |
11.1 ± 4.3 |
0.001 |
|
Hemoglobin, g/dL |
13.4 ± 1.5 |
14.7 ± 1.5 |
0.019 |
|
Platelets, ×103/mm3
|
217.4 ±74.9 |
217.5 ± 105.9 |
0.999 |
|
C-reactive protein, mg/dL |
0.7 ± 1.6 |
0.9 ± 0.9 |
0.68 |
|
Blood urea nitrogen, mg/dL |
10.6 ± 3.4 |
62.6 ± 51.9 |
< 0.001 |
|
Creatinine, mg/dL |
0.53 ± 0.3 |
3.9 ± 3.2 |
< 0.001 |
|
Creatine kinase, IU/L |
5,298.3 ± 9,533.6 |
59,787.4 ± 49,644.4 |
< 0.001 |
|
Myoglobin, ng/mL |
979.0 ± 1,831.0 |
12,843.6 ± 1,560.7 |
< 0.001 |
|
Hematuria |
29 (26.1) |
6 (75.0) |
0.003 |
|
Proteinuria |
22 (19.8) |
6 (75.0) |
< 0.001 |
Table 3.
Multivariate logistic regression for the application of renal replacement therapy
|
Variable |
Adjusted odds ratio (95% confidence interval) |
P value |
|
Blood urea nitrogen |
11.41 (0.00-1,889,130.81) |
0.691 |
|
Creatinine |
1.03 (0.93-1.13) |
0.598 |
|
Creatine kinase |
1.06 (1.00-1.12) |
0.036 |
|
Myoglobin |
1.13 (0.85-1.51) |
0.402 |
References
1. Costa Azevedo A, Costa E Silva A, Juliana Silva C, Poço Miranda S, Costa M, Martinho I. Benign acute childhood myositis: a 5-year retrospective study. Arch Pediatr 2022;29:490–3.   4. Harmer MJ, Nijloveanu V, Thodi E, Ding WY, Longthorpe C, Fenton-Jones M, et al. Paediatric rhabdomyolysis: A UK centre's 10-year retrospective experience. J Paediatr Child Health 2023;59:346–51. 5. Ozawa H, Noma S, Nonaka I. Myositis and rhabdomyolysis with influenza infection. Nihon Rinsho 2000;58:2276–81. 13. Garg RK, Malhotra HS, Jain A, Malhotra KP. Dengue-associated neuromuscular complications. Neurol India 2015;63:497–516. 14. Park IH, Kim YA, Shin SY, Park YS, Yoon HJ, Kim CO, et al. A case of dengue fever complicated by rhabdomyolysis. Infect Chemother 2005;37:234–6. Korean.
15. Gelbart B, DeMarco R, David Hussey A, Namachivayam SP, McRae R, Quinlan C, et al. Rhabdomyolysis in a tertiary PICU: a 10-year study. Pediatr Crit Care Med 2018;19:e51–7.
Appendices
Appendix 1
Causing microbes*
|
Variable |
Total (N = 145) |
BACM (N = 69) |
Rhabdomyolysis (N = 76) |
P value |
|
Influenza |
70 (48.3) |
31 (44.9) |
39 (51.3) |
0.835 |
|
Coronavirus disease 2019 |
11 (8.6) |
7 (10.1) |
4 (5.3) |
0.175 |
|
Parainfluenza |
7 (4.8) |
0 (0) |
7 (9.2) |
0.019 |
|
Enterovirus |
5 (3.4) |
1 (1.4) |
4 (5.3) |
0.276 |
|
Rhinovirus |
4 (2.8) |
1 (1.4) |
3 (3.9) |
0.443 |
|
Streptococcus spp. |
3 (2.1) |
3 (4.3) |
0 (0) |
0.048 |
|
Dengue virus |
3 (2.1) |
1 (1.4) |
2 (2.6) |
0.711 |
|
Astrovirus |
1 (0.7) |
0 (0) |
1 (1.3) |
0.376 |
|
Bocavirus |
1 (0.7) |
0 (0) |
1 (1.3) |
0.376 |
|
Respiratory syncytial virus |
1 (0.7) |
0 (0) |
1 (1.3) |
0.376 |
|
Rotavirus |
1 (0.7) |
0 (0) |
1 (1.3) |
0.376 |
|
Salmonella spp. |
1 (0.7) |
0 (0) |
1 (1.3) |
0.376 |
|
Not detected |
37 (25.5) |
25 (36.2) |
12 (15.8) |
0.191 |
|
|















