Introduction
Iliopsoas abscess (IPA), a collection of pus involving the iliopsoas muscle, is a rare disease in neonates and infants (1). Owing to its rarity, a high index of suspicion is important for timely diagnosis and treatment (2-4). The 3 most common symptoms of neonatal IPA are fever, inguinal swelling or discoloration, and limited lower limb movement (3,5-7). If the symptom triad is present, ultrasonogram (US), computed tomography, or magnetic resonance imaging (MRI) should be performed to diagnose IPA (3).
We present a case of IPA in an 82-day-old boy who presented with fever without localizing signs and was initially hospitalized for presumptive diagnosis of urinary tract infection (UTI). This study was approved by the institutional review board at Hanyang University Hospital with a waiver for informed consent (IRB no. 2023-06-039).
Case
An 82-day-old boy visited the emergency department (ED) with fever lasting for 3 days as the only symptom. Initial vital signs were as follows: heart rate, 160 beats/minute; respiration rate, 40 breaths/minute; and temperature, 38.1 ℃. No abnormalities were found in physical and neurological examinations. He was delivered by elective cesarean section at a gestational age of 38 weeks with a birth weight of 3,000 g. His mother had no relevant medical history at the time of delivery. Laboratory findings showed a white blood cell count of 27.4 × 103/µL with 64.3% segmented neutrophils and C-reactive protein concentration of 15.7 mg/dL. Urinalysis, which used the urine collected with a urine bag, showed 5-9 cells/high-power field. The boy was hospitalized to treat UTI as a presumptive diagnosis and given cefotaxime.
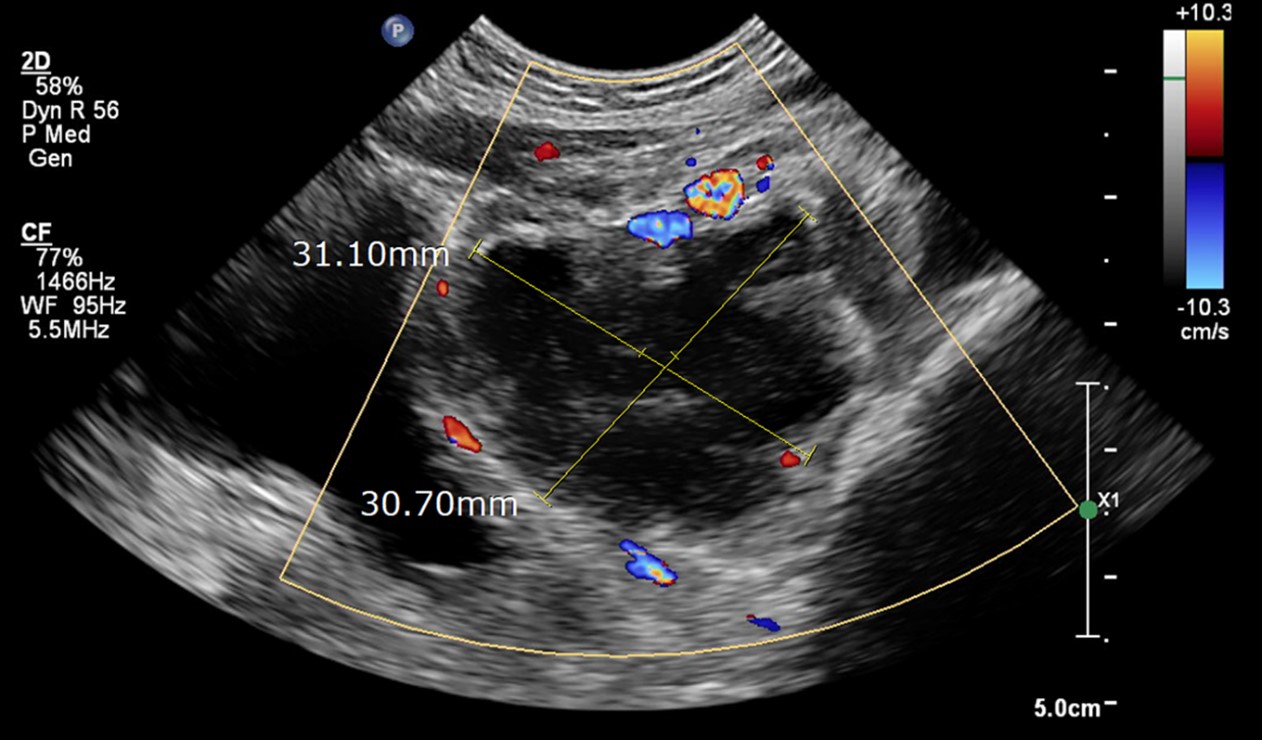
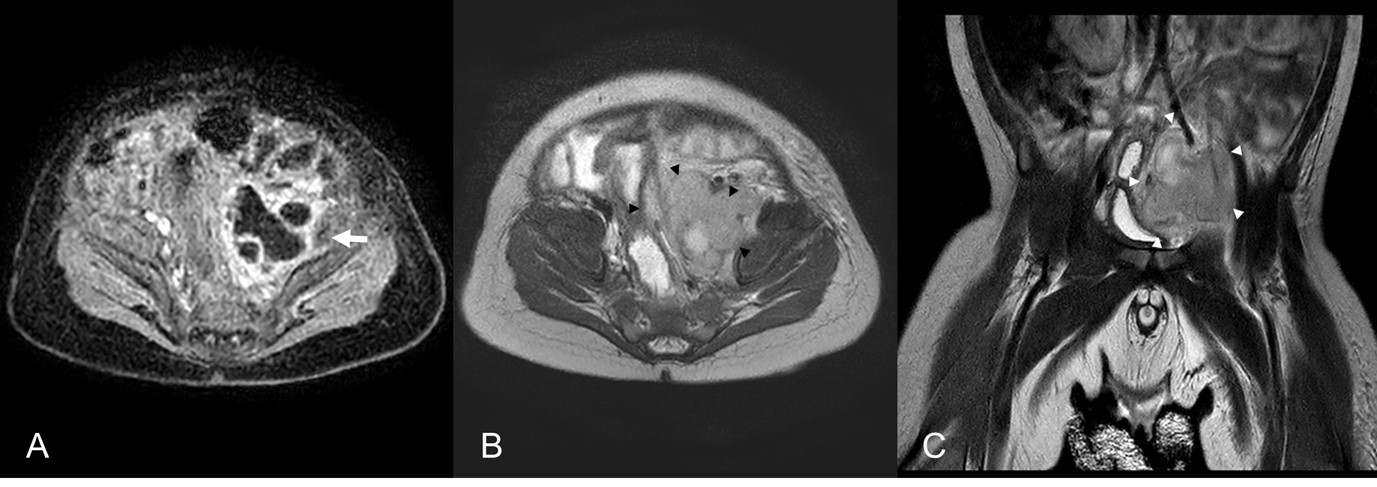
After hospitalization, 50,000 colony-forming units/mL of Streptococcus agalactiae, which was susceptible to cefotaxime, were identified in the urine. Despite the absence of pyuria on a follow-up urine and antibiotic therapy, fever persisted until day 3. An abdominal US was performed to evaluate the cause of the fever, showing a 3.1 cm-sized hypoechoic lesion occupying the left pelvis (Fig. 1). On the same day, an MRI suggested that the pelvic mass was a left IPA (Fig. 2). Considering the imaging finding, vancomycin was added to cover a possible involvement of Staphylococcus aureus, the most commonly identified pathogen in IPA (1,4,8-10). On day 4, we inserted a pigtail catheter for percutaneous drainage and immediately drained 5 mL of thick purulent pus. On day 6, blood culture was found to be negative, and the fever subsided.
On day 7, a follow-up US showed a decrease in the size of IPA. Methicillin-sensitive S. aureus was isolated with the drained pus. On day 11, the draining catheter was removed. On day 14, the follow-up laboratory findings showed a white blood cell count of 11.9 × 103/µL and C-reactive protein concentration of < 0.3 mg/dL. On the same day, the boy was discharged uneventfully. He had been well without any symptoms until 15-month follow-up.
Discussion
Owing to its rarity in infants, IPA is seldom suspected as a differential diagnosis at the initial presentation (2,7). In 2014, the first case of neonatal IPA was reported in Korea, and approximately 20 cases of neonatal IPA have been reported in English literature (1). Imaging tests, including US, computed tomography, and MRI, are performed to detect IPA if the infant has the abovementioned symptom triad. In the present case, there were no symptoms other than fever. Thus, it was difficult to suspect IPA at the ED. UTI was initially suspected given the initial pyuria, and later S. agalactiae were found in the urine. However, the persistent fever prompted performing US. The US showed the pelvic mass, which was confirmed as IPA on MRI. Based on the MRI findings and pus culture, we consider that the infant boy had a primary IPA due to methicillin-sensitive S. aureus with secondary UTI, which was developed by extrinsic compression of the urinary bladder. After the surgical drainage and broad-spectrum antibiotic therapy, he was discharged uneventfully.
Our case is unique because the infant boy had no localized groin symptoms, which have been reported in previous literature (1-7,9-13). To our best knowledge, most literature regarding neonatal IPAs shows that patients consistently had localizing signs, such as inguinal swelling or discoloration (1-7,9-13). The localized signs of IPA develop when the abscess spreads inferiorly to the inguinal area (14). However, reviewing the MRI findings (Fig. 2), the abscess was extending into the pelvic cavity, rather than spreading inferiorly. We assume that the location of the IPA might have resulted in the absence of groin symptoms.
Regarding treatment, antibiotic therapy alone is usually insufficient, and surgical drainage is needed in most cases (2,4,5,7,10). In the present case, the fever persisted despite the antibiotic therapy during the first 3 days. If the imaging tests had not been performed, the detection of IPA would have been delayed, predisposing the infant boy to complications, such as sepsis (2,9). For early detection and appropriate treatment, the possibility of IPA should be considered in infants presenting with intractable fever without localizing signs.
Neonatal or infant IPA is a rare disease difficult to diagnose without the symptom triad (7). The present case suggests that IPA can occur in young infants without the classic inguinal swelling or discoloration. Infants having fever without localizing signs frequently undergo physical examination, laboratory tests, urinalysis, blood culture, or cerebrospinal fluid profile in EDs. If these tests do not identify the cause of fever, or if the fever persists despite the antibiotic therapy, additional imaging tests should be promptly performed to find IPA.