서론
소아 다기관염증증후군(multisystem inflammatory syndrome in children, MIS-C)은 중증급성호흡증후군 코로나바이러스-2(severe acute respiratory syndrome coronavirus 2, SARS-CoV-2) 감염 후 면역반응으로 인한 다기관 염증이 특징이고, 여러 계통을 침범하여 쇼크로 진행할 수 있으므로 진단이 지연되면 치명적일 수 있다(1-3). 최근 단면 연구에 따르면 MIS-C는 70% 이상에서 아프리카 또는 히스패닉계에서 발생하지만(2,4,5), 인종적 차이보다 코로나바이러스병-19(coronavirus disease 2019, COVID-19) 환자 수가 발생률에 영향을 줄 수 있다(6). 가와사키병과 유사한 임상양상을 보이지만 병태생리 및 경과가 다르므로, 이 병이 흔한 아시아에서 감별진단이 특히 중요하다(7). 한국에서는 2021년 7월 7일 현재 신고 사례 16건 중 6건이 MIS-C로 확인됐고(8), COVID-19가 풍토병으로 전환되어 역학조사 및 진단검사가 줄었다. 그러나, 소아·청소년은 무증상 또는 경증 감염이 흔하고 성인보다 예방 접종률이 낮으므로, 응급진료 시 MIS-C 가능성을 고려해야 한다.
이에 본 저자는 조절되지 않는 열, 구토, 전신 발진으로 방문하여 MIS-C로 의심하고 진단한 후 적절히 치료한 증례를 경험했기에 문헌고찰과 함께 보고하는 바이다. 본 연구는 본원 임상연구심의위원회의 승인을 받고 시행했다(IRB no. 2023-04-013).
증례
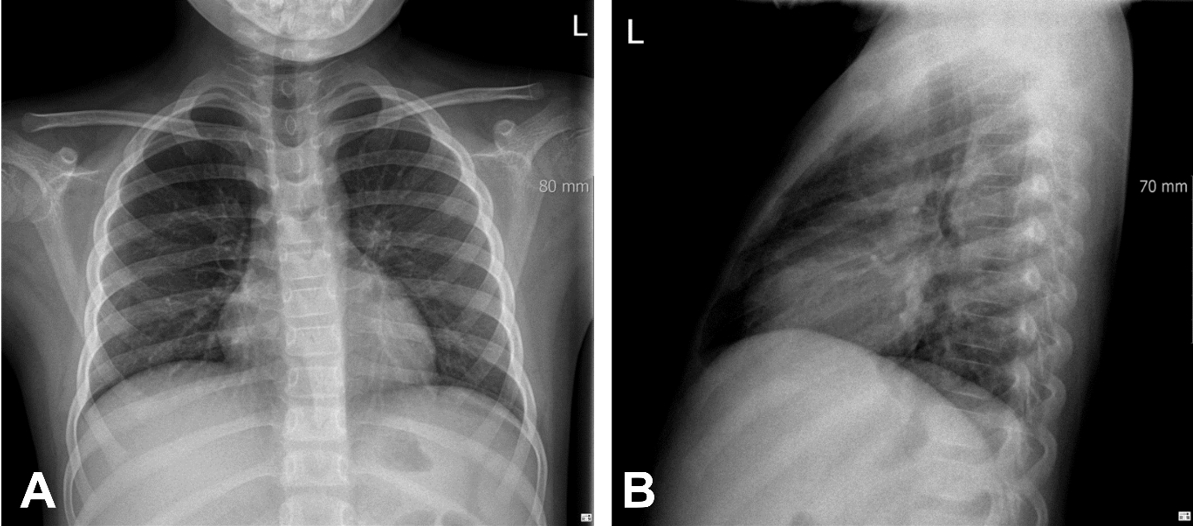
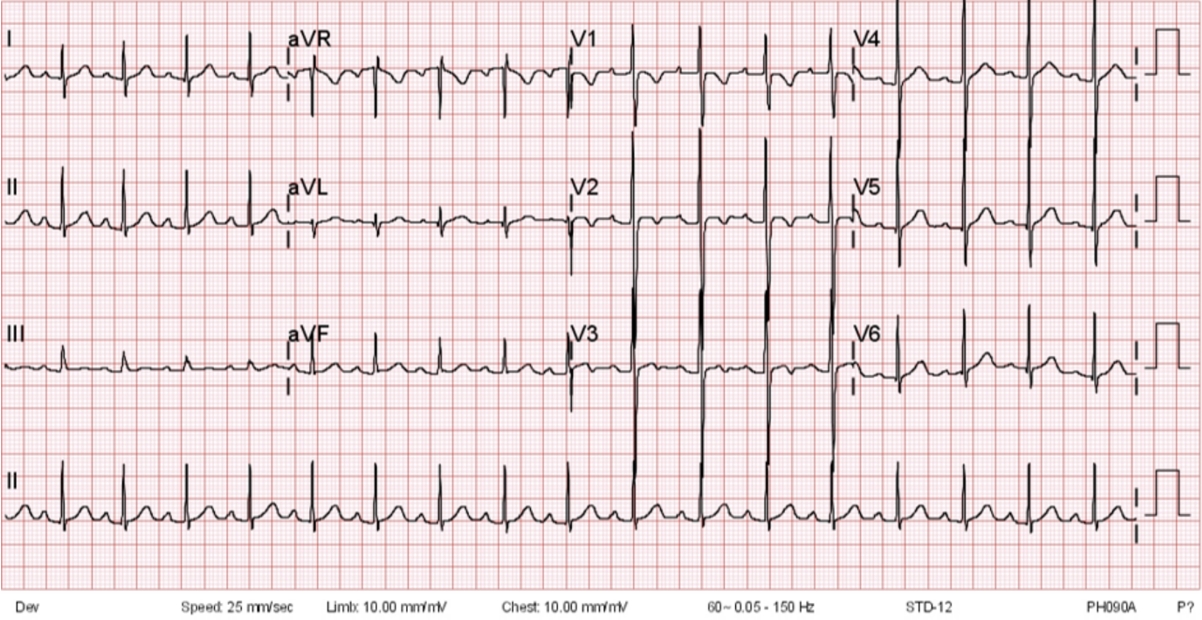
2022년 2월, 평소 건강하던 7세 남자가 열, 구토, 전신 발진으로 본원 응급실을 방문했다. 방문 4일 전부터 열이, 3일 전부터 구토 및 전신 발진이 각각 발현하여 소아청소년과 일차의료기관에 입원했다. 이후 양쪽 결막충혈, 인두 발적이 관찰되어 가와사키병을 추정 진단으로 정맥내 면역글로불린을 투여했으나 증상이 지속하고 저혈압을 동반하여 본원으로 이송됐다. 본원 방문 당시 의식은 명료했으나 처져 있었고, 활력징후는 혈압 92/67 mmHg, 심박수 117회/분, 호흡수 28회/분, 체온 38.1 ℃, 산소포화도 98%였다. 환자는 구역 및 복통을 호소했으며 배와 팔다리에 다형(polymorphic) 발진을 보였다. 신체검사에서 양쪽 결막충혈이 있었으나 목 림프절은 만져지지 않았고, 배 전체에 통증이 있으나 압통은 없었으며 양쪽 손 및 다리에 통증을 동반한 발적 및 부종을 보였다. 방문 당시 확인한 검사실 소견은 Table 1에 요약했다. 일반영상, 심전도, 응급현장 초음파(point-of-care ultrasound)에서 특이 소견은 없었다(Figs. 1, 2). 정맥내 결정질 용액 및 해열제 투여 후 측정한 혈압은 118/75 mmHg였다. SARS-CoV-2, 호흡기(19종) 및 수막염 바이러스(6종)에 대한 중합효소사슬반응 및 인플루엔자 A, B 신속항원검사는 모두 음성이었다. 제1병일에 채혈하여 제 2병일에 확인한 페리틴 농도 433 ng/mL (참고치: 9.9-71.7 ng/mL) 및 트라이글리세라이드 농도 282 mg/dL (참고치: < 50 mg/dL)를 근거로, 면역글로불린 저항성 가와사키병으로 추정 진단하여 소아청소년과에 입원했다. 제2병일에 열이 지속하여 methylprednisolone과 aspirin을 투여했고, 제4병일에 시행한 SARS-CoV-2 혈청검사에서 G면역글로불린 양성으로 확인되어 COVID-19 연관 MIS-C로 진단하고 methylprednisolone (15 mg/kg)을 투여했다. 심장초음파검사에서 양쪽 심실 기능은 정상이었고 관상동맥 지름은 좌주간부(left main coronary artery) 관상동맥 2.9 mm (Z-score = -0.18), 좌전하행동맥(left anterior descending coronary artery) 2.3 mm (Z-score = -0.33), 우관상동맥(right coronary artery) 2.6 mm (Z-score = 0.39)였다. 제6병일부터 열 및 발진이 호전됐으며 적혈구침강속도, C반응단백질, 페리틴 수치도 감소하여, 제12병일에 합병증 없이 퇴원했다.
고찰
2020년 영국에서 처음 보고된 MIS-C는 중증으로 진행하면 신속한 면역조절제(immunomodulator) 요법이 필요하지만, 비특이적 임상증상 및 검사실 소견으로 인해 초기에 단순 COVID-19으로 오인하여 진단이 지연되기 쉽다(1). MIS-C의 병태생리는 정확히 밝혀지지 않았지만, 인터루킨-1β, 6, 8, 10, 17, 종양괴사인자-α, 인터페론-γ 등 사이토카인이 상승하는 과다 염증 반응이 내피세포 기능장애 또는 미세혈관병증을 유발하여, 결과적으로 조직 손상 또는 장기부전을 유발한다(9,10). 미국 질병관리본부의 표준 진단 기준에 따르면, MIS-C는 21세 미만, 24시간 이상 지속하는 원인 미상 열 환자가 검사실 검사에서 염증이 확인되고, 심혈관계, 신장, 호흡계, 혈액, 소화계, 피부, 신경계 중 2개 이상 기관을 침범해야 한다(11). 가와사키병과 유사하지만 70%-90%에서 구역, 구토, 복통, 설사 등 소화계 증상을 동반하며 좌심실기능 저하, 저혈압, 쇼크 등이 잘 발생한다. 특히 MIS-C의 호발 연령은 6-11세(중앙값: 8.3세)로, 가와사키병보다 더 많은 나이에 발생한다(5,12). 따라서, 저혈압 또는 소화계 증상을 동반한 소아⸱청소년 열 환자가 응급실을 방문한 경우, MIS-C를 염두에 두고 진단 계획을 세워야 한다. 본 증례의 환자는 7세였고, 구역, 구토, 복통을 호소했으며 혈액 및 점막피부 침범을 확인하여 MIS-C를 의심하고 추가 검사 및 입원을 결정했다. 특징적 검사실 소견으로 림프구 감소, 중성구 증가, 혈소판 감소가 가장 흔하고, 저나트륨혈증, 저알부민혈증을 보일 수 있으며, 아미노기전달효소, D이합체, C반응단백질, 적혈구침강속도, 페리틴, 프로칼시토닌, 젖산탈수소효소 수치가 증가할 수 있다. Capone 등(13)에 따르면, MIS-C는 SARS-CoV-2에 노출된 후 초기에 약한 M면역글로불린 반응보다 중⸱후기에 나타나는 항 스파이크 단백질 G면역글로불린(anti-spike protein immunoglobulin G) 반응과 연관되므로, 노출 3-6주 후에 발병한다. 이에 따라 MIS-C 환자에서 20%-40%만 SARS-CoV-2 중합효소사슬반응 양성으로 나오며, 양성으로 나오더라도 대개 cycle threshold 값이 높다. 반면 혈청검사는 80%-90%에서 양성이므로, MIS-C가 의심되면 G면역글로불린 농도를 확인하는 것이 도움이 된다.
MIS-C의 치료가 정립되지는 않았지만, 저혈압 교정을 포함한 환자 감시 및 지지요법을 시작하면서 중증의 경우 정맥내 면역글로불린 및 스테로이드를 단계적으로 사용하는 면역조절제 요법이 필요하다(14-16). 특히 심혈관계 증상이 빨리 진행하여 쇼크 등 치명적 경과로 진행하는 것을 막기 위해 신속한 치료를 시작해야 한다(14-16). 특히, 정맥내 면역글로불린 투여 2일 후까지 열이 조절되지 않으면, 스테로이드를 병용하는 것이 효과적이다. MIS-C는 열, 염증표지자 수치, 혈역학적 불안정성이 호전되면 대체로 좋은 예후를 보인다(17). 본 증례에서도 외부 병원에서 면역글로불린을 투여했으나 열이 지속하여 스테로이드를 추가 투여했고, 쇼크로 진행하지 않아 체외막산소공급 등 추가 치료 및 합병증 없이 퇴원할 수 있었다.
원인 미상 열을 주요호소증상으로 응급실을 방문하는 환자의 진료에는 MIS-C에 대한 높은 수준의 인식과 임상적 추론을 통해 초기에 진단⸱치료하는 것이 예후에 중요하다. 특히, 6세 이상에서 원인 미상 열이 지속하면서 가와사키병에서 볼 수 있는 점막피부, 소화계, 심혈관계 침범을 동반하는 경우, 적극적으로 MIS-C를 진단하기 위한 검사를 시행하고 신속한 치료를 위한 협진이 필요하다.