발작을 동반한 급성 저나트륨혈증으로 방문하여 수정토에 의한 소장폐색증으로 진단된 12개월 여자 환자
Small bowel obstruction by water beads in a 12-month-old girl presenting with acute hyponatremia with seizure
Article information

Trans Abstract
Although foreign body ingestion is relatively common in children aged 6 months-3 years, small bowel obstruction rarely develops, and few cases require surgical interventions. We report a case of 12-month-old girl who presented to the emergency department with new-onset seizure after projectile bilious vomiting. The initial diagnosis was seizure caused by hyponatremia based on laboratory findings, plain abdominal radiograph, brain magnetic resonance imaging, and electroencephalography. Despite fluid resuscitation, clinical manifestations did not improve, and severe ileal obstruction was found on computed tomography. Emergency laparoscopy showed a foreign body (a water bead [superabsorbent polymer], 3 cm in diameter) that was subsequently removed by enterotomy. After the surgery, bilious vomiting continued, and gastrografin did not pass on fluoroscopy. The second laparoscopy showed a residual foreign body that was crushed and then removed by minimal enterotomy. She was discharged in good condition 5 days after the second surgery. This case suggests a particular danger of water beads as foreign bodies and the need for differential diagnosis of multiple foreign bodies in children with poor communication skills.
서론
이물 섭취는 6개월-3세 소아에서 발생 빈도가 높다[1]. 이중 약 10%-20%은 내시경을 통해 제거되고, 수술적 제거가 필요한 경우는 1% 미만이다[2].
수정토는 흡수성이 강한 고분자 물질로, 대부분의 이물이 소장을 빠져나가는 것과 달리 물과 접촉하면 부피가 30-60배 이상 증가한다[3]. 최근 수정토(superabsorbent polymer ball, water beads)가 수경용 식물 재배나 방향제, 촉감놀이 등의 재료로 널리 이용되고 있다. 본 저자는 수정토를 삼킨 뒤 장폐색증 및 저나트륨혈증에 의한 발작을 보인 12개월 여자 환아의 증례를 보고하고자 한다. 본 연구는 본원 임상연구심의위원회의 승인을 받고 시행했다(IRB No. CUH 2019-09-033).
증례
발작 과거력 없는 12개월 여자 환아가 구토로 외부 병원에 입원했다가 다음 날 발작이 발생하여 본원 응급실로 이송됐다. 구토는 식사 2-3시간 후 처음 발생했으나 외부 병원에서 치료적 금식 중에도 분출성 담즙 구토 양상으로 반복했다. 외부 병원에서 전신 강직간대발작이 발생하여 15분간 지속하다가, diazepam 3 mg 정맥내투여 후 진정됐다. 이후 수액(0.2% 염화나트륨 + 포도당 40 g/L) 800 mL를 주입했다. 키 80.0 cm (95백분위수), 체중 9.7 kg (50백분위수)이었다.
응급실 방문 직후 의식은 진정 상태로 초기 활력징후는 혈압 80/50 mmHg, 호흡수 22회/분, 심장박동수 132회/분, 체온 36.6℃, 산소포화도 98%였다. 신체검사에서 동공반사와 심부건반사는 정상이었으며 바빈스키 징후는 없었다. 복부는 경도의 팽만을 보였으나 부드러웠고 장음은 감소했다. 간헐적 복통이 있었으나 압통 및 반동압통은 없었고, 간비장비대 및 복부 종괴는 만져지지 않았다. 경부 및 흉부에서 이상 소견은 없었으며 사지의 부종은 없었다.
혈액검사에서 백혈구 4,080/μL, 혈색소 10.6 g/dL, 혈소판 154,000/μL, C-반응단백질 0.03 mg/L (참고치: 0-0.5 mg/L)였고, 나트륨 117 mEq/L, 칼륨 3.7 mmEq/L, 염화물 89 mEq/L, 혈당 139 mg/dL, 칼슘 9.3 mg/dL (참고치: 8.8-10.8 mg/dL), 인 3.7 mg/dL (참고치: 3.8-6.5 mg/dL), 혈액요소질소 6 mg/dL, 크레아티닌 0.18 mg/dL, 알라닌아미노전달효소 28 IU/L, 아스파르테이트아미노전달효소 58 IU/L였으며, 요검사에서 농뇨, 혈뇨, 단백뇨는 없었다. 요비중은 1.006, 혈청 삼투질농도 274 mOsm/kg (참고치: 289-308 mOsm/kg), 소변 삼투질농도 71 mOsm/kg (참고치: 300-900 mOsm/kg)였고, 소변 나트륨은 15 mmol/L이었다. 임상증상, 이송 전 주입된 수액, 검사 결과를 근거로 발작이 위장관 손실과 저장액 주입에 의한 저나트륨혈증에 기인한 것으로 추정하고 3% 염화나트륨(9 mL/hr, 2시간 동안)을 투여했다. 이후 혈액검사에서 나트륨 124 mEq/L로 호전되어 0.9% 염화나트륨으로 교체했다. 뇌 자기공명영상검사와 뇌파도에서 이상 소견은 없었다.
입원 첫날 시행한 복부 단순방사선사진 상복부 외 부위에서 가스가 거의 보이지 않아(Fig. 1A) 장폐색증을 의심하고 복부초음파를 시행했다. 장중첩증은 없었으며, 좌하복부에서 소장벽 비후와 함께 내강 확장 및 소량의 복수가 있었다. 이에 위장관염에 의한 장폐색증으로 추정하고 치료했으며, 호전되지 않으면 복부 컴퓨터단층촬영을 시행할 계획이었다. 환아는 금식 및 수액요법으로 전해질이상이 교정됐고, 제2병일 오전에 구토 및 장음이 호전되어 점심부터 연식을 공급했다. 같은 날 저녁 식사 3시간 후 분출성 담즙 구토가 발생하여 시행한 복부 단순방사선사진 장폐색증을 확인하고(Fig. 1B), 다시 금식을 시행했다. 제3병일, 다시 담즙 구토가 있어 시행한 컴퓨터단층촬영에서 회장에 심한 장폐색증이 확인되어(Fig. 1C, D), 제4병일에 응급 복강경 탐색술을 시행했다. 수술 중 회장 근위부에서 종괴를 확인하고(Fig. 2A) 배꼽절개부위로 장을 꺼내 절개하여 직경 약 3 cm의 원형 수정토 1개를 제거했다(Fig. 2B). 수술 후 구토는 없었으며 제7병일 저녁부터 식이를 시도했으나 이튿날 담즙 구토가 4회 발생하여 금식을 시행하며 제9병일에 가스트로그라핀 투시검사를 시행했다. 검사 결과 소장이 확장되어 있고 조영제가 투여 12시간 후와 17시간 후에도 확장부위 하방으로 내려가지 못하고 여전히 남아있는 것을 확인했다(Fig. 3A, B). 제10병일에 2차 복강경 수술을 시행한 결과, 1차 수술 부위로부터 15 cm 하방에 위치한 회장 병소를 배꼽절개부위로 꺼내고 장절개는 최소한으로 하여 수정토 1개를 으깨어 제거했다(Fig. 3C). 또한 전체 소장을 탐색하여 잔류이물이 없는 것을 확인했다. 2차 수술 후 3일째에 가스 배출 및 배변을 확인했고, 환아는 추가 구토 없이 식이 진행이 원활하여 수술 5일 후 퇴원했다.

Findings from plain abdomen radiographs and computed tomography performed before the first surgery. On day 1, plain abdomen radiograph showed a dilated stomach with very little gas in the distal bowels (A). On day 2, plain abdomen radiograph showed a stepladder sign (B). On day 3, computed tomography showed dilated small bowel loops on a coronal view (C) and decompressed small bowel distal to the obstructive lesion on axial view (arrow, D).
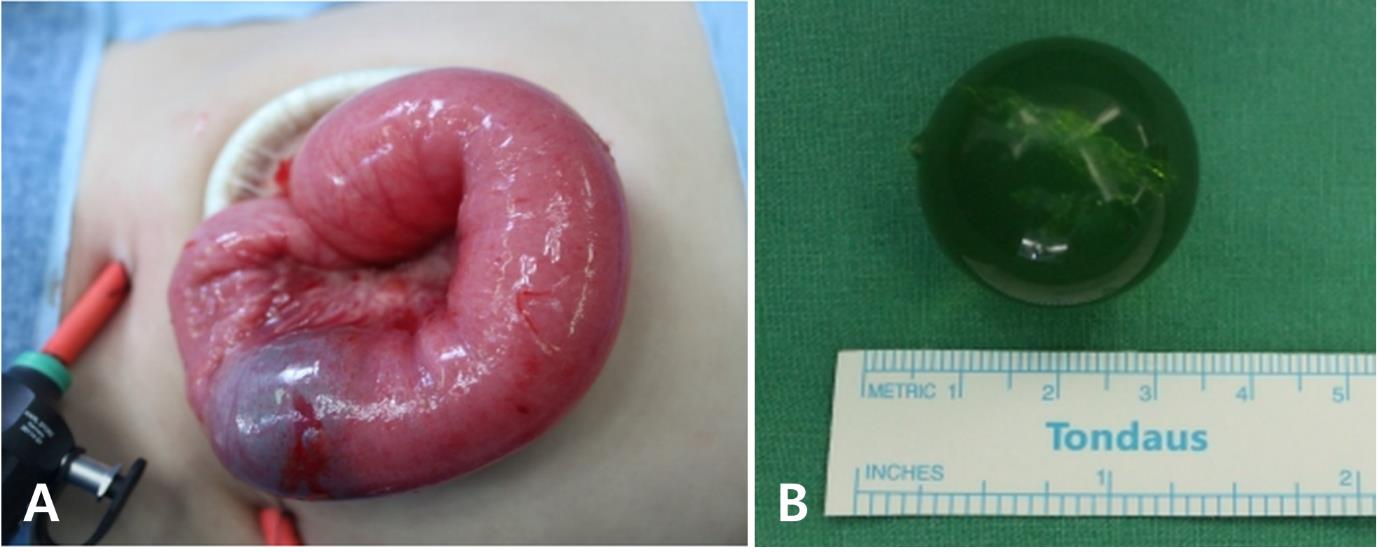
The first foreign body obstructing the proximal ileum with a clear transition point and decompressed distal bowel (A). The extracted water bead (superabsorbent polymer), of which diameter was 3 cm (B).

Plain abdomen radiographs before the second surgery and laparoscopic finding of a second foreign body during reoperation. The radiograph (day 9) showed dilated small bowel loops (12 hours after the ingestion of gastrografin) (A). The contrast remained within the small bowel (17 hours after ingestion) (B). The second foreign body found in the ileum, 15 cm below where the first one was located (C).
고찰
소아 이물 섭취의 약 40%는 보호자가 인지하지 못하며, 전체 이물 섭취의 약 90%는 무증상으로 시간이 지나면 자연 배출된다[4,5]. 하지만 이물 섭취로 장폐색증, 천공, 출혈, 샛길 등 합병증이 발생할 수 있다[6].
최근 수정토를 수경용 식물 재배나 방향제, 촉감놀이 등의 재료로 널리 이용하는데, 건조한 상태의 수정토는 크기가 작고(2-3 mm), 사탕과 비슷한 모양으로 어린 소아가 이를 삼킬 위험이 있다. 또한, 보호자가 섭취 사실을 인지하더라도 작은 크기 때문에 위험성을 간과하기 쉽다. 하지만 수정토는 물에 접촉하면 골프공 크기까지도 부피가 증가 할 수 있어 자연 배출이 어렵고 어린 소아에서 장폐색증을 초래할 위험이 매우 높다[7,8].
본 증례는 환아가 수정토를 삼킨 것을 보호자는 알지 못했으며, 부피가 커진 수정토가 장폐색증을 유발했으나 단순방사선사진, 초음파, 컴퓨터단층촬영에서 이물을 시사하는 특징적 병소가 없어 진단에 어려움이 있었다. 수정토가 유문을 통과하기 전 작은 크기를 유지하다가, 시간 경과와 함께 물과 접촉이 증가하여 크기가 빠르게 증가하여 회장폐색증을 일으킨 것으로 추정한다[9]. 수정토의 크기에 염분, pH, 온도가 영향을 미친다[10]. 저나트륨혈증은 삼투질농도 감소를 통해 수정토가 커지는 데에 기여하며, 특히 증류수 접촉 시 최대 크기 증가를 보인다고 알려졌다[11]. 또한 pH 2 미만에서 크기 증가가 없다가 pH 증가에 따라 크기가 증가하는 경향을 보인다[10]. 본 증례 환아는 삼투질농도가 낮은 상황에서, pH가 2 미만인 위를 거쳐 소장을 지나면서 pH 증가에 따라 수정토 크기가 급격히 증가하면서 장폐색증을 일으킨 것으로 추정한다.
수정토 섭취 후 수술적 치료를 시행한 사례들이 문헌으로 보고됐다(Table 1) [3,6-9,12-13]. 본 증례의 특징은 환아가 수정토 두 개를 섭취했으나 병력 및 검사 결과에서 이를 확인하지 못하여, 결과적으로 두 차례의 수술로 장폐색증을 치료할 수 있었다는 점이다. 이는 의사소통이 어려운 어린 소아에서 이물 섭취에 의한 장폐색증 뿐 아니라, 2개 이상의 이물 섭취 가능성을 고려해야 함을 시사한다.

Clinical manifestations in reported cases of water bead ingestion including the current case
본 증례에서는 수정토 섭취 환아가 수술을 통해 치료됐다. 수정토 연관 장난감 제작은 말레이시아, 영국, 이탈리아에서 금지됐는데[13], 이는 섭취 시 매우 심각한 위험이 있기 때문일 것이다. 따라서 앞으로 제조업체에서 수정토를 섭취 시 위험에 대한 경고문구를 기재하는 것을 의무화하거나 소아의 손이 닿기 어려운 방식으로 제작하고, 장난감 용도로는 사용을 규제하는 등의 노력이 필요하다.
Notes
이해관계
본 저자는 이 논문과 관련된 이해관계가 없음.