오스트레일리아 단일 이차수련병원 응급실에 두통으로 방문한 소아환자의 뇌 컴퓨터단층촬영 비율
What are the head computed tomography scan rates in children presenting with headache to an Australian community teaching hospital emergency department?
Article information

Trans Abstract
We aimed to determine head computed tomography (CT) scan rate in the children presenting with non-traumatic headache who visited an Australian community teaching hospital emergency department. This was a planned substudy of an investigation of the epidemiology of headache in children presenting to the emergency department. A total of 225 children were studied; 6 underwent CT scan (CT scan rate, 2.7%; 95% confidence interval, 1.2-5.7). No intracranial pathology was identified. The rate was much lower than previously reported. The optimal CT scan rate for children presenting with headache remains unclear and is worthy of further research.
Headache is a chief complaint for about 1% of pediatric emergency department (ED) attendances [1-4]. Most cases have benign causes, but serious causes, such as central nervous system infections and brain tumours, are also possible. Previous studies from freestanding children’s hospitals show that the proportion of children with serious diagnoses accounts for 4%-6% [1,2]. Computed tomography (CT) scan rates in children presenting to EDs with headache have been reported variably, ranging from 10% [1-3] to 40% [4]. However, these studies were all performed in paediatric EDs, and outside Australia; 2 in the United States and 1 each in Taiwan and Italy. Paediatric EDs are likely to have a different population. Particularly, they are likely to have more patients with known serious pathology, such as tumours or ventriculoperitoneal shunts that creates bias in their results. There is also evidence that the rate of CT scan as part of headache evaluation in ED is rising, at least in the United States, with the rate rising from 11.6% to approximately 30% between 1995 and 2008 [5]. We aimed to determine head CT scan rate in the children with headache who visited an Australian community teaching hospital ED.
This was a planned substudy of a study investigating the epidemiology, treatment and outcome of children presenting to ED with headache. It was a retrospective study by medical record and radiology report review conducted at Sunshine Hospital ED, an adult-paediatric ED in a university-affiliated general hospital, in Western Melbourne, Australia. It has an annual paediatric census of approximately 25,000. Inclusion criteria were: presentation between January 1 and December 31, 2016 with a major symptom of non-traumatic headache and age 2-16 years. Exclusion criteria were: a history of head injury within the previous 48 hours, a ventriculoperitoneal shunt in situ or known intracranial conditions associated with headache, such as tumour, abscess, and mass. Data collected included demographics, investigation, treatment, and disposition. The outcome of interest was the rate of head CT scans as part of the ED work-up. This descriptive study was approved by the institutional ethics committee (WHLREP QA2017.73). Consent was not required for data collection.
A total of 225 children were studied with a median age of 9 years (interquartile range, 6-13 years). Clinical features and final diagnosis are shown in Table 1. Six children underwent CT scan (CT scan rate, 2.7%; 95% confidence interval, 1.2-5.7). Four scans were normal and 2 showed sinusitis. No intracranial pathology was identified. Other studies have also reported sinusitis as among the most common abnormal findings on CT [2,3].
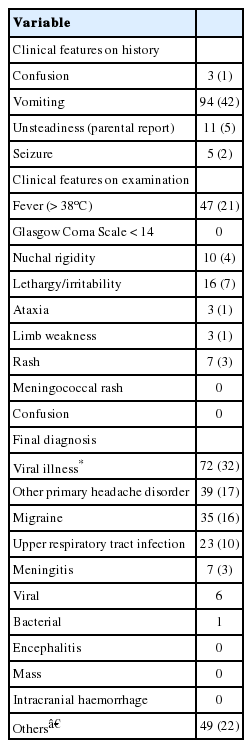
Clinical features and outcome of the participants (n = 225)
The CT scan rate in the children presenting with headache who visited the Australian ED was much lower than has been reported in other settings. This could reflect differences in the study populations, as most of the previous data were derived from paediatric EDs in freestanding children’s hospitals. Only 1 study performed in a general hospital reported a 10% CT scan rate and a 1.5% intracranial pathology rate [3]. However, the study had different inclusion and exclusion criteria, making direct comparison impossible. There were also differences in inclusion criteria of the other studies, as some of them also included children who had sustained a minor head injury without loss of consciousness. We do not consider that these differences could explain the significant variations on CT scan rates. There is no robust data addressing what the optimal CT scan rate should be in children with headaches or the reasons for geographical differences. We believe that a rate closer to the lower end of the range is appropriate in children without high-risk clinical features. It would balance risk of missed serious diagnosis with the risk of ionizing radiation-induced cancer. This is supported by the findings of Gandhi et al. [6] that for children with primary headache and a normal neurological examination, the rate of abnormal CT findings was very low, and therefore CT rarely altered diagnosis or management.
Limitations of this study are as follows. It is single centre-based and thus may not be generalizable. Data was collected retrospectively, so some might be missed. Some patients might be missed due to miscoding of presenting complaint.
In conclusion, the head CT scan rate in the children with non-traumatic headache who visited an Australian community teaching hospital ED was much lower than previously reported in other settings, and no intracranial pathology was identified. The optimal CT scan rate for children with headache remains unclear and is worthy of further research.
Notes
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
Acknowledgements
No funding source relevant to this article was reported.