소아응급실에서 복통의 처치
Management of abdominal pain in pediatric emergency departments
Article information

Trans Abstract
Abdominal pain is one of the common complaints among children who visit pediatric emergency departments (PEDs), but aggressive management has been proven insufficient. Physicians working at PEDs must know the principles of abdominal pain management, especially the dose, lower age limitation, and adverse effects of each drug. Through this review of published literature, I would like to suggest future study topics, and aid to establish the Korean guidelines for the management of abdominal pain in PEDs.
서 론
복통은 소아응급실을 방문하는 가장 흔한 원인 중 하나로, 한국에서 10세 이상 소아응급환자 주증상의 15% 이상을 차지한다[1]. 복통 환자에서 가장 중요한 것은 외과복증을 감별하는 것이며, 더불어 통증에 대한 처치를 하는 것이 중요하다. 그러나 환자의 나이에 따라 사용할 수 있는 약이 제한적이며, 표준 용량에 맞춰 사용한다고 하더라도 기대한 효과가 발생할지 여부와 부작용 발생에 대한 우려가 크다. 마약성 진통제를 사용하는 경우, 보호자 입장에서는 거부감을 느끼고 의료진 입장에서는 통증 감소가 진단을 방해할 수 있다고 걱정한다. 이 때문에, 응급실에서 복통 환자의 진통요법이나 퇴원 약 처방에 대해 어려움이 있다.
대부분의 문헌은 복통에 대해 응급질환 여부 및 해당 질환의 진단에 필요한 내용을 주로 다루며, 흔한 비응급질환인 급성위장염 및 기능성 위장장애의 진통요법을 기술한 경우는 드물다. 본 종설에서는 문헌 고찰을 통해 응급실에서 흔하게 접하는 급성위장염 및 기능성 위장장애를 중심으로, 안전하고 효율적인 복통의 처치를 다루고자 한다. 이를 통해 소아응급환자의 복통의 처치, 특히 소아응급실에서 필요한 효과적이고 효율적인 연구 방향을 제시하고, 한국 실정에 맞는 복통 처치의 지침 개발에 도움을 주고자 한다.
본 론
1. 복통의 병태생리 및 평가
복통은 병태생리에 따라, 내장-, 체성-, 연관- 통증으로 구분한다. 내장통증은 무디고 쑤시는 비 국소적 통증으로, 해당 기관의 신경 분포에 해당하는 피부분절에서 인지되므로 통증 부위가 질환 부위와 다를 수 있다. 체성통증은 날카롭고 지속되는 국소적 통증으로 내장의 염증이 벽쪽복막에 전달되어 나타난다. 연관통증은 위장관 외 장기가 복벽-척수 감각로(sensory pathway)를 공유하는 데에 기인하며, 대표적인 예로 폐렴이나 요로감염에 의한 복통이 있다.
통증 강도를 객관적으로 평가하여 이를 진단 및 진통요법의 판단 기준으로 삼는 것은 응급실에서 매우 중요하다[2]. 6세 미만 환자는 의사 전달 능력이 부족하므로, 그림을 이용한 통증 척도(예: Wong-Baker FACES pain scale)를 주로 사용한다[3]. 그러나 나이 또는 개인 별로 다른 발달의 정도에 따라 통증 표현 방식이 다양할 뿐 아니라 주양육자와 의료진 간 의사소통 또한 통증의 평가에 영향을 미치므로, 통증 강도를 객관적으로 평가하여 처치를 하는 것은 쉽지 않다. 그 결과 소아환자의 통증에 대한 처치가 불충분할 뿐 아니라 성인에 비해 오히려 중요하지 않게 인식되고 있다[4].
2. 비(非)약물 요법
기능성 위장장애에서 고섬유질 식이는 효과가 없으며, partially hydrolyzed guar gum은 장내세균의 프리바이오틱스로 작용하여 반복 복통과 과민대장증후군에서 효과적으로 보고됐다[5-7]. 제거 식이요법(elimination diet)에서 유당 제거 식이는 논란이 있으나, 자두(프룬 등), 콩류, 우유, 밀 등을 피하는 low fermentable oligosaccharides, disaccharides, monosaccharides and polyols diet는 과민대장증후군에서 효과가 있었다[8].
급성위장염의 식이 요법은, 모유 수유아는 모유 수유를 지속하고, 분유 수유아는 입원하거나 설사가 1주 이상 지속하는 경우 유당제거분유를 권장하는 것이다[9].
통증 감소를 위해, 보호자가 안고 있거나 환자가 좋아하는 자세를 취하도록 유도하거나, 영아에겐 설탕 또는 공갈젖꼭지, 포대기로 단단하게 감싸기, 좋아하는 소리 들려주기, 피부 접촉 등의 방법을 사용할 수 있다[10,11]. 신경인성 대장 기능 이상이나 변비 환자에 대한 일부 연구에 따르면 복부 마사지가 통증 감소에 효과적이라고 보고되었으나, 추가 연구가 필요하다[12,13].
프로바이오틱스는 장관 장벽 기능, 병원체에 결합 및 저해 작용, 장 염증반응 조절 등의 기전으로 위장관에 유익한 역할을 하며, 장벽 과민 반응을 줄여주는 작용도 한다[14,15]. 기능성 위장장애, 과민대장증후군, 기능성 변비, 영아산통 등에 일부 효과가 있다는 보고가 있으나, 최근 급성위장염 소아 연구에서 설사나 구토의 평균 기간, 유치원 결석, 가정 내 전염 등에 영향이 없는 것으로 조사되어 다양한 종류의 균주, 용량, 치료 기간 등에 대한 지속적인 연구가 필요하다[15-19].
3. 약물 요법
외과복증은 배제할 수 있으나 정확한 진단이 확실치 않다면, 증상에 중점을 두고 초기 치료를 시행한다. 상부위 장관 질환에 의한 복통이 소화불량을 동반하면, 대부분의 의사가 만성 상부위장관 질환 치료와 유사하게 위산억제제를 가장 많이 사용한다는 보고가 있다[20]. 기능성 변비 환자에서는 관장을 주요한 처치 중 하나로 고려해야 한다. 급성복통 환자 중 기능성 변비가 차지하는 비율은 약 25%이고, 중등도 이상의 복통을 유발하기도 하며, 약 70%에서 관장을 시행한 것으로 보고됐다[21]. 변비와 관련이 없는 하부 위장관질환에 의한 복통 중 경련성이고 광범위한 통증이 있는 환자에게는 항연축제(antispasmodics) 투여를 고려한다[22]. 초기 진통요법 후 재평가와 추적 관찰은 반드시 필요하다.
1) 비마약 진통제
Acetaminophen (paracetamol)은 해열 작용과 함께 경도의 진통 작용이 있으며 미숙아에 대한 연구도 있을 만큼 소아에서 안전한 약이다. 2011년 미국 식품의약품안전청은 정맥내주사용제를 2세 이상 소아환자의 통증에 대해 마약성 진통제와 병행 투여 및 해열 등 목적으로 허가했다. 빠른 작용이 필요하거나 경구 투여가 어려울 때 유용하지만, 비용 측면을 고려해야 한다[23]. 급성위장염으로 인한 탈수 소아환자에서 ibuprofen을 사용한 경우, 대부분 경증이거나 자연 치유되었지만 54%에서 급성신부전을 초래하는 것으로 보고되어 주의가 필요하다[24].
비스테로이드소염제로 ibuprofen, naproxen, diclofenac, etodolac, meloxicam, celecoxib 등이 있는데, ketorolac은 정맥내주사용제가 있으며, 액상 ibuprofen은 항문으로 투여할 수 있다. 한 가지 약으로 효과가 불충분하면 다른 비스테로이드소염제를 추가 투여할 수 있다. 투여 용량과 주의점은 Table 1을 참고한다.
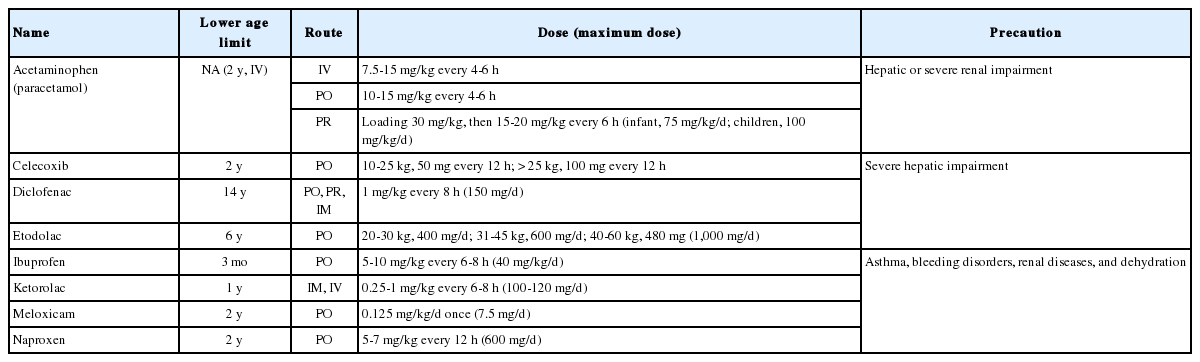
Non-opioid analgesics for children and adolescents
2) 마약성 진통제
중증도 이상의 통증에는 마약성 진통제가 효과적이다. 최근 연구에 따르면, 급성복통 소아환자에서 morphine 투여(0.1 mg/kg/dose)는 외과복증의 진단에 영향을 주지 않으며 통증 감소에 효과적이고 안전하지만[25-27], 마약성 진통제는“마약”이라는 용어에서 오는 거부감과 중독이나 호흡억제와 같은 부작용에 대한 우려로 인해 사용이 적은 실정이다. 그러나 이런 부작용은 과량 투여 시 나타나고, 소아환자에서 중독에 대한 영향은 극히 미미한 것으로 알려졌다. 다만 소아에 대한 연구가 적으므로, 특히 2세 미만에서 주의가 필요하며, codeine은 12세 미만 소아에서 수면 무호흡증이 있거나 편도절제 후에는 금기이다[28-32]. 소아에서 사용 가능한 마약성 진통제는 Table 2를 참고한다.
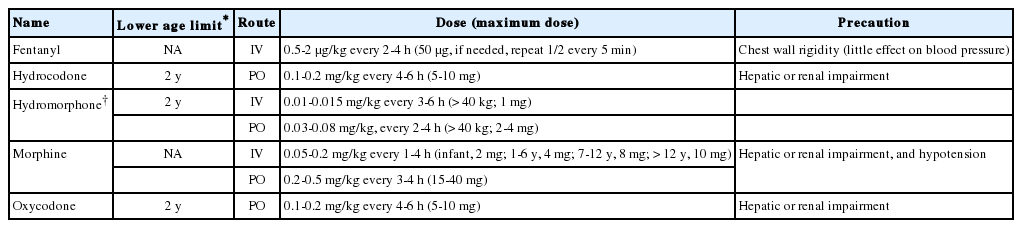
Opioid analgesics for children and adolescents
3) 소화기관 용제
기능성 위장장애에 사용하는 대부분의 약은 효과가 증명되지 않았으며 효과가 있다고 보고한 연구는 소규모이거나 연구방법이 부적절한 경우가 많으므로 주의해서 사용한다[33,34].
항연축제 중 peppermint oil은 과민대장증후군 소아환자에서 복통의 기간과 빈도를 감소시키고 부작용이 없어 사용을 권고한다[35]. Mebeverine은 위장관 평활근에서 항연축작용을 하는 것으로 알려졌지만, 소아환자에서는 통계적으로 유의한 효과가 없는 것으로 보고되었다[36]. Trimebutine, mosapride, metoclopramide, domperidone, itopride 등과 같은 위장운동촉진제도 효과적이라는 보고가 있으나, 연구방법이 부적절하여 효과를 확신할 수 없다[37,38].
복통을 동반한 기능성 위장장애는 불안 또는 우울과 관련되므로, 항우울제를 사용할 수 있다. Amitriptyline은 저용량(10-30 mg) 투여 시, 신경계에 작용하여 통증의 역치를 낮추어 청소년기 과민대장증후군에 효과적이며 부작용도 거의 없는 것으로 알려졌다[39]. Citalopram (20 mg/d) 또한 만성 반복성 복통 소아환자에서 효과적이다[40].
항히스타민제인 cyproheptadine은 칼슘통로차단제로 항세로토닌 효과가 있어 만성 반복성 복통, 소화불량, 복통과 관련된 기능성 위장장애 소아환자에서 효과적이라는 보고가 있다[41,42]. 그러나, 연구설계가 부적절하고 효과 면에서도 통계적 유의성에 문제가 있어, 효과에 대해서는 아직 부정적이다.
H2수용체차단제 중 famotidine은 반복성 복통 소아환자에서 복통의 호전은 없었으나 소화불량과 관련된 전체적인 증상 호전을 보여 일부 효과는 있는 것으로 추정한다[43]. 이외에도 ranitidine, cimetidine, omeprazole 등도 소화불량을 개선하지만 보다 체계적인 연구가 필요하다[44].
이 외에 melatonin, 칼슘통로차단제인 flunarizine, 세로토닌 길항제인 pizotifen, 항생제인 rifaximin, cotrimoxazole 등에 대한 보고가 있으나 연구가 제한적일 뿐 아니라 대부분 효과도 불확실하다[33].
결 론
응급실을 방문하는 소아 복통 환자에 대해 보다 적극적인 통증 조절에 대한 관심이 필요하다. 특히 나이에 적합한 진통제의 종류, 약 용량, 부작용을 숙지하는 것이 필요하다. 또한, 다기관 및 전문가 그룹 연구를 통해, 한국 실정에 맞는 복통 처치 지침을 개발해야 한다.
Notes
이해관계
본 저자는 이 논문과 관련된 이해관계가 없음.
Acknowledgements
본 저자는 이 논문과 관련된 재정지원을 받지 않았음.