급성위장염 소아환자에서 ondansetron 경구요법 시행 후 정맥내 수액요법 빈도 및 응급실 체류시간의 변화
Changes in intravenous hydration frequency and emergency department length of stay after implementation of oral ondansetron therapy in children with dehydration due to acute gastroenteritis
Article information
Trans Abstract
Purpose
Oral ondansetron is a safe and effective antiemetic drug to facilitate oral rehydration therapy in acute gastroenteritis (AGE) with mild dehydration. We investigated the effect of oral ondansetron therapy on intravenous (IV) hydration frequency and emergency department length of stay (EDLOS) in dehydrated children with AGE.
Methods
We reviewed 15,813 children aged 12-60 months with primary diagnosis of AGE who visited a tertiary care university-affiliated hospital emergency department. The enrolled children were divided into the pre- (from January 2009 to June 2011) and post- (from January 2016 to June 2018) ondansetron groups according to the implementation of oral ondansetron therapy in the emergency department. As primary outcomes, IV hydration frequency, EDLOS, and hospitalization rate were compared between the 2 groups. As secondary outcomes, EDLOS and hospitalization rate were compared between the children in the post-ondansetron group who underwent the therapy, and those who did not.
Results
Of 7,990 enrolled children, 3,300 (41.3%) were designated as the post-ondansetron group, and among them 1,093 (33.1%) underwent oral ondansetron therapy. This group showed a lower IV hydration frequency, a shorter median EDLOS compared to the other group (61.9% vs. 55.8%, P < 0.001; 223.0 minutes vs. 175.0 minutes, P < 0.001, respectively), and a higher hospitalization rate (7.9% vs. 9.9%, P < 0.001). The children in the post-ondansetron group who underwent the therapy showed a shorter median EDLOS and a lower hospitalization rate compared to those who did not (142.0 vs 205.0 minutes, P < 0.001; 2.9% vs. 13.4%, P < 0.001, respectively).
Conclusion
Oral ondansetron therapy may reduce IV hydration frequency and EDLOS in dehydrated children with AGE, and can be considered in those having severe vomiting.
서론
급성위장염은 소아에게 가장 흔한 질병 중 하나로, 세계적으로 연간 130만 명이 이 질환으로 사망하며 이 중 5세 이하가 약 50만 명을 차지한다[1]. 탈수 및 전해질 불균형 교정이 중요하며, 경증 및 중등도 탈수를 보이는 환자의 초기 치료로 경구수액요법이 권장된다[2]. 하지만, 급성위장염 소아환자(환자)의 70%가 호소하는 구토가 경구수액요법의 성공을 방해한다[3,4]. 이 환자군에서 ondansetron 요법은 구토를 호전시켜 경구수액요법의 성공을 유도할 수 있다[5-10].
하지만, 급성위장염 환자에서 ondansetron 경구요법이 정맥내 수액요법 빈도 및 응급실 체류시간에 미치는 영향에 대해선 논란이 있다[11,12]. 또한, 한국에서 급성위장염 환자에서 ondansetron 경구요법은 비급여로 시행되고 처방 빈도가 낮으며 관련 연구도 부족한 실정이다.
본 저자는 구토를 주 증상으로 본원 응급실을 방문한 급성위장염 환자를 ondansetron 경구요법 시행 전후 시기로 나눠 정맥내 수액요법 빈도, 응급실 체류시간, 입원율의 변화를 분석하고자 연구를 진행했다. 본 연구는 의학연구윤리심의위원회의 승인을 받고 진행했다(AJIRB-MED-MDB-18-269).
대상과 방법
1. 연구대상자
본원은 연간 약 33,000명의 환자가 방문하며, 성인 환자를 포함하여 연간 약 87,000명이 방문하는 한국 경기 남부의 권역응급의료센터이다. 본원 응급실에서는 2011년부터 구토를 주 증상으로 방문한 급성위장염 환자를 대상으로 ondansetron 경구요법과 함께 경구수액요법을 병합해 시행하고 있다. Ondansetron 설상정을 체중에 따라(8-14 kg, 2 mg; 15-30 kg, 4 mg; > 30 kg, 8 mg) 투여하고, 투여 15-20분 후에 경구수액요법을 시행한다[5]. 경구수액요법은 경증 및 중등도 탈수 환자를 대상으로 시행한다. 정맥내 수액요법은 중증 탈수 환자는 대상으로 시행하는 것을 원칙으로 하되, 중등도 탈수 환자 중 심한 설사, 아파 보이는 외양, ondansetron 경구투여에도 지속하는 구토가 있으면 시행한다.
본원 응급실을 방문해 응급실 퇴실 진단으로 급성위장염(국제질병분류-10 코드: A09.0, A09.9, A09.9A, A09.9C)을 부여받은 12-60개월 환자 중 주 증상이 구토인 환자를 연구대상자로 정의했다. 단, 심한 설사, 마비성 장폐색증, 중환자실 입원 및 수술, 전원, 불충분한 자료를 가진 환자는 제외했다. 연구대상자의 나이 12-60개월은 기존 연구 결과, 본원에서 사용 중인 경구수액제제의 조성, 말초정맥내 카테터 삽입의 난이도에 근거한 것이다.
방문시기에 따라 두 군으로 나누어, ondansetron 경구요법 시행에 따른 정맥내 수액요법 빈도, 응급실 체류시간, 입원율을 비교했다. 2009년 1월부터 2011년 6월에 방문한 환자는 전 ondansetron 군으로, 2016년 1월부터 2018년 6월에 방문한 환자는 후 ondansetron 군으로 각각 정의했다(각 30개월). 2011년 7월부터 2015년 12월은 ondansetron 경구요법을 의료진에게 교육 및 피드백하던 시기로, 해당 요법의 영향을 분석하기 어려워 연구기간에서 제외했다.
2. 연구방법
의무기록을 조사해 환자의 나이(월) 및 성별, 정맥내 수액요법 및 ondansetron 경구요법 시행 여부, 응급실 체류시간, 입원 여부를 수집했다. 본 연구의 1차 결과(primary outcome)로서 정맥내 수액요법의 시행 빈도, 응급실 체류시간, 입원율을 두 군 간에 비교하고자 했다. 2차 결과(secondary outcome)로서 후 ondansetron 군에 속한 환자의 ondansetron 경구요법 시행에 따른 응급실 체류시간 및 입원율의 차이를 분석하고자 했다.
3. 통계적 분석
SPSS ver. 15.0 (SPSS Inc, Chicago, IL)을 이용했다. 연속형 변수는 정규분포 여부에 따라 Student t-test 또는 Mann-Whitney U test를, 범주형 변수는 chi-square test 또는 Fisher exact test를 각각 이용했다. P가 0.05 미만인 경우를 통계적 유의성이 있는 것으로 정의했다.
결과
1. 일반적 특성
연구기간에 본원 응급실을 방문한 192,681명 중, 2009년 1월부터 2011년 6월에 109,540명이, 2016년 1월부터 2018년 6월에 83,141명이 각각 방문했다. 급성위장염 진단 코드로 선별된 15,813명 중 7,823명을 제외하고, 최종적으로 전 ondansetron 군 4,690명, 후 ondansetron 군 3,300명을 연구대상자로 등록했다(n = 7,990) (Fig. 1). 후 ondansetron 군 3,300명 중 1,093명(33.1%)이 ondansetron 경구요법을 경험했다. 전 ondansetron 군 환자 나이의 중앙값(28.0개월)은 후 ondansetron 군 환자 나이의 중앙값(32.0개월)보다 유의하게 적었다(Table 1).
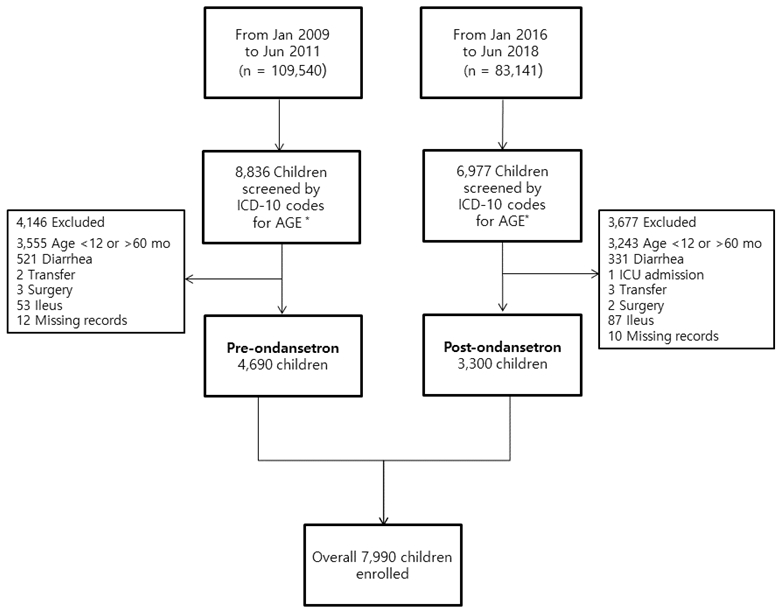
Flowchart depicting the selection of the study children. *A09.0, A09.9, A09.9A, and A09.9C. ICD: International Statistical Classification of Diseases and Related Health Problems, AGE: acute gastroenteritis, ICU: intensive care unit.

Comparison of IV hydration frequency, EDLOS, and hospitalization rate between the pre- and post-ondansetron groups (n = 7,990)
2. Ondansetron 경구요법 시행 전후 정맥내 수액요법 빈도, 응급실 체류시간, 입원율의 변화
본 연구에서 1차 결과 중 정맥내 수액요법 시행 빈도와 응급실 체류시간은 후 ondansetron 군에서 유의하게 감소했다(61.9% vs. 55.8%, P < 0.001; 223.0 [85.0-402.5] vs. 175.0 [111.0-288.0]분, P < 0.001). 반면, 입원율은 같은 군에서 유의하게 증가했다(7.9% vs. 9.9%, P < 0.001) (Table 1).
후 ondansetron 군 환자를 ondansetron 경구요법 시행에 따라 분석한 결과, ondansetron 투여 환자에서 유의하게 짧은 응급실 체류시간(142.0 [111.0-208.0] vs. 205.0 [111.0-317.0]분, P < 0.001)과 낮은 입원율(2.9% vs. 13.4%, P < 0.001)을 보였다(Table 2).

Comparison of EDLOS and hospitalization rate between the children in the post-ondansetron group who underwent the combination therapy of oral ondansetron and oral rehydration solution, and those who did not (n = 3,300)
고찰
본 연구는 구토를 주 증상으로 응급실을 방문한 급성위장염 환자에서 ondansetron 경구요법이 정맥내 수액요법 빈도 감소 및 응급실 체류시간 단축과 연관됨을 보여준 첫 한국 연구이다. 한국 소아응급의료에서 ondansetron 경구요법이 보편화하지 못한 점을 고려하면, 비록 단일기관 연구이지만 환자 7,990명의 경험을 보고한다는 의미도 있다.
2014년 Freedman등[11]은 후향적 다기관연구를 통하여 ondansetron 경구요법에 따른 정맥내 수액요법 빈도를 분석한 결과, ondansetron 경구요법이 많이 증가한 시기에 정맥내 수액요법의 빈도가 17.8%로 그 이전 시기의 18.7%와 비교하면 큰 영향을 주지 못한 것으로 보고했다. 그러나 이 연구에 나타난 추가분석에 따르면, 정맥내 수액요법을 시행한 전체 환자의 13.4%가 ondansetron 경구요법을 경험했고, 연구에 참여한 일부 병원에서는 ondansetron 경구요법 빈도가 증가한 후 정맥내 수액요법 빈도가 감소했다. 이에 Freedman등[11]은 ondansetron 경구요법을 경구수액요법이 실패할 수 있는 환자를 대상으로 시행해야 함을 제시했다. 또한 Rutman 등[12]은, 2005년부터 응급실을 방문한 경증 및 중등도 탈수 환자에서 경구수액요법 도중 구토 시, 경구수액요법을 20분간 중단하고 이후 구토 지속하면 정맥내 수액요법을 시행하는 지침을 제시했다. 이 지침의 시행만으로 정맥내 수액요법 빈도가 48%에서 44%로 감소했으며, 2015년부터 중등도 탈수 시 ondansetron 경구요법 추가 이후 정맥내 수액요법 빈도가 26%로 감소했다[12].
본 연구에서 조사한 정맥내 수액요법 시행 빈도는 ondansetron 경구요법 시행 후 유의하게 감소했으나, 그 감소 폭은 비교적 작았다. Freedman 등[6]의 연구에 참여한 환자의 나이는 평균 3.4세였고, Rutman 등[12]은 18세 이하 환자를 대상으로 연구를 진행했다. 반면, 본 연구에서 전후 ondansetron 군 환자 나이의 중앙값은 각각 28, 32개월이었다. 본 연구는 탈수 또는 전해질 불균형 발생 우려가 큰 어린 환자를 다수 포함하여 정맥내 수액요법 시행 빈도가 비교적 높았던 것으로 추정한다.
Ondansetron 경구요법 시작 전후의 입원율은 후 ondansetron 군에서 더 높았다. 이 환자 중 33.1%가 ondansetron 경구요법을 경험했음에도 불구하고, 정맥내 수액요법 빈도의 감소 폭은 6.1%로 비교적 작았다. 비록 탈수의 중증도를 객관적으로 비교하지 못했지만, 후 ondansetron 군 환자의 입원율이 상대적으로 높았던 점으로 미루어 이 군에서 탈수 중증도가 더 높았을 수 있다. 즉, 후 ondansetron 군 환자의 높은 탈수 중증도가 정맥내 수액요법 빈도의 감소 폭이 작았던 것에 영향을 미쳤다고 해석할 수 있다. 전 ondansetron 군에서 정맥내 수액요법 시행 빈도가 비교적 높았던 것은, 본원 의료진 또는 보호자의 정맥내 수액요법 선호도와 연관될 수 있다. 이 추론은 의료진이 탈수 치료를 위해 경구보다 정맥내 수액요법을 선호한다는 보고와 일맥상통한다[13,14].
본 연구에서 응급실 체류시간이 ondansetron 경구요법 시행 이후 유의하게 감소한 것은 기존 연구와 일치하며, 그 절댓값도 비교적 짧았다. Rutman 등[12]에 따르면 경증 및 중등도 탈수를 보이는 급성위장염 환자에서 전술한 지침 시행 후 평균 응급실 체류시간이 250분에서 60분 감소했고, 이후 ondansetron 경구요법 시행으로 20분이 더 감소했다. Freedman 등[6]도 ondansetron 경구요법 시행 증가에 따라 평균 응급실 체류시간이 8.6시간에서 5.9시간으로 감소했다고 보고했다. 연구기간에 응급실 체류시간에 영향을 미칠 수 있는 본원 응급실 전문의의 인원 및 직접 진료 비율은 변화가 없었다.
후 ondansetron 군에서 ondansetron 경구요법 시행 빈도는 33.1%로, 급성위장염 환자 중 경증 또는 중등도 탈수로 경구수액요법을 시도하는 빈도가 늘었음을 알 수 있다. 이 33.1%의 환자는 유의하게 짧은 응급실 체류시간과 낮은 입원율을 보였다. Ondansetron 경구요법은 비용 및 보험 문제, 낮은 약 인지도로 인해 사용 빈도가 낮은 실정이다. 하지만, 상기 결과는 구토가 주 증상인 급성위장염 환자에게 ondansetron 경구요법을 통해, 경구수액요법이 성공할 기회를 늘리고 나아가 정맥내 수액요법 시행과 응급실 체류시간, 입원율을 줄이는데 기여할 수 있음을 뒷받침한다.
본 연구는 몇 가지 제한점이 있다. 첫째, 후향적 연구설계 때문에 탈수 정도를 비교하기 어려웠다. 파악하지 못한 탈수 중증도의 차이가 결과에 영향을 미쳤을 수 있다. 이 제한점을 고려하여, 본 저자는 각 군의 연구기간으로 30개월로 정의하여 가급적 다수의 환자를 확보하고자 했고, 1차 결과로 전체 응급실의 정맥내 수액요법 시행 빈도를 제시했다. 둘째, ondansetron 경구요법을 경험한 환자의 재방문 및 약 부작용 빈도를 분석하지 못했다. 셋째, 본원 의료진의 정맥내 수액요법 선호도가 연구 결과에 영향을 미쳤을 수 있다. 이러한 제한점을 보완하려면, 전향적 다기관 연구가 필요하다.
본 연구는 구토를 주 증상으로 응급실을 방문한 급성위장염 환자에게 ondansetron 경구요법을 시행함으로써 침습적인 정맥내 수액요법 빈도 및 응급실 체류시간을 줄일 수 있음을 시사한다. 따라서, 심한 구토로 경구수액요법을 시행하기 어려운 급성위장염 환자에게 ondansetron 경구요법을 고려할 수 있다.
Notes
이해관계
본 저자는 이 논문과 관련된 이해관계가 없음.
Acknowledgements
본 저자는 이 논문과 관련된 재정지원을 받지 않았음.