몬테카를로 시뮬레이션을 이용한 finger counting method 정확도평가
Validation of the finger counting method using the Monte Carlo simulation
Article information

Trans Abstract
Purpose
The dose of drug and the size of instrument are determined based on children’s weight. We aimed to validate the finger counting method (FCM) for weight estimation in Korean children using the Monte Carlo simulation.
Methods
We estimated the weight of Korean children aged 1 to 9 years by the FCM. These measurements were compared with the weight extracted by the Monte Carlo simulation applied to the “2007 Korean Children and Adolescents Growth Standard.” Pearson correlation coefficients (r) were measured to assess the correlation between the weight extracted by the simulation and that estimated by FCM. Bland-Altman analyses were performed to assess the agreement between the weight extracted by the simulation and that estimated by FCM and 2 other well-known pediatric weight estimation formulas (the Advanced Pediatric Life Support and Luscombe formulas).
Results
Data regarding 9,000 children’s weight selected by age and gender was randomly extracted using the simulation. We found a positive correlation between the weight estimated by the FCM and the weight extracted (in boys, r = 0.896, P < 0.001; in girls, r = 0.899, P < 0.001). The FCM tended to underestimate weight in the children aged 7 years or old.
Conclusion
This article suggests the usefulness of FCM in weight estimation, particularly in children younger than 7 years. With appreciation of the limitation in older children, the FCM could be applied to emergency practice.
서론
2015년 응급의료통계연보에 따르면, 10세 미만 소아응급환자(소아환자)는 연간 1,621,348명으로 전체 응급환자의 약 16%를 차지했다[1]. 소아응급진료에서 약물 용량과 기구 크기는 주로 환자의 체중을 근거로 결정되므로, 체중을 파악하는 것은 응급진료에 있어서 중요하다. 하지만, 응급상황에서 체중을 측정하거나, 당황한 의료진 또는 보호자가 체중을 정확하게 추정하기는 어렵다[2]. 이 같은 상황에서는 신속∙정확한 체중 추정 방법이 필요하다.
여러 연구자가 다양한 소아 체중 추정 방법을 검토했다[3-7]. 주로 소아환자의 나이, 키, 체형 등을 이용하여 임의의 나이에 따라 나타나는 체중과의 연관을 파악하여 공식을 유도하고, 이를 다수의 다른 환자에 적용함으로써 정확도를 평가하는 연구가 많았다. 최근 개발된 체중 추정 방법인 finger counting method (FCM)는 공식 대신 양 손가락으로 간단하게 체중을 추정할 수 있고 정확도가 다른 방법보다 떨어지지 않으므로, 응급상황에서 적용하기 쉽다[8]. 그러나 이 방법에 대한 정확도평가가 부족하다. Broselow tape의 정확도평가 연구도 표본수가 작은 경우가 많았고, 특히 한국 소아환자의 인종적 특성을 반영하지 못했다[9-11].
이에 본 저자는 “2007년 소아청소년 표준성장도표(표준성장도표)”를 근거로, 몬테카를로 시뮬레이션으로 임의의 모집단을 추출하고, 이를 이용하여 한국 소아환자에서 FCM의 정확도를 평가하고자 했다[12].
대상과 방법
1. 한국 소아 체중의 정상범위
표준성장도표는 한국 소아의 체중, 키, 혈압의 정상범위를 제시하며, 각 변수의 5-95백분위수를 정상으로 정의한다. 이 ‘정상’은 정책적 용어로, 일종의 선별기준이다. 본 연구에서는 나이에 따른 체중의 5-95백분위수를 체중 정상범위(정상범위)로, 이를 벗어나는 체중을 비정상으로 각각 정의했다. 본 연구는 대중에게 공개된 정보를 이용하는 연구로, 연구대상자에 대해 대면, 조작, 개인정보 수집을 수반하지 않았다. 한림대학교 성심병원 임상연구심사위원회는 이러한 특성을 고려하여, 본 연구에 대한 심의를 면제했다(IRB No. 2017-I119).
2. 몬테카를로 시뮬레이션을 이용한 체중 추출
실측 체중을 근거로 체중 추정 방법의 정확도를 평가하려면, 충분한 표본수의 소아환자를 대상으로 체중을 직접 측정하여 FCM을 이용한 추정 체중과 비교하는 것이 바람직하다. 이 과정에 많은 시간과 노력이 필요하므로, 본 연구에서는 컴퓨터를 이용한 몬테카를로 시뮬레이션을 이용했다. 이 시뮬레이션은 2차 세계대전 중 원자폭탄 개발을 위해 최초로 이용했고, 실험의 진행이 현실적으로 어려운 경우 적용할 수 있다는 장점 때문에 최근 자연과학, 공학, 사회과학 등에서 많이 사용한다[13-15].
표준성장도표에 기재된 체중을 성별에 따라 구분하고, 1-9세를 1년 간격으로 나눈 나이별 정상범위를 정의했다. 월령으로 세분된 나이별 정상범위에서 중앙값에 해당하는 5-6개월의 체중을 나이 및 성별에 따른 대표값으로 정의했다. 이후 나이별 정상범위에서 컴퓨터를 이용하여 특정 분포를 따르지 않는 난수를 1,000개씩 발생시켜, 이 난수의 값을 실제 소아환자의 체중으로 가정하여 추출했다. 이 시뮬레이션을 통해 총 9,000개의 체중을 추출했다.
3. 비교대상 방법의 체중 추정
FCM은 왼손 엄지부터 새끼손가락 순으로 1, 3, 5, 7, 9세로 정의하고 오른손 엄지부터 손가락부터 새끼손가락 순으로 10, 15, 20, 25, 30 kg으로 정의함으로써, 나이별 체중을 추정하는 방법이다. 1-9세에서 짝수 나이는 해당 나이의 앞뒤 홀수 나이별 체중의 평균으로 추정했다(예: 4세, 17.5 kg).
FCM과 비교하기 위해, 나이를 이용한 대표적인 체중 추정 방법인 Advanced Pediatric Life Support (APLS) 공식(1-10세, 체중[kg] = [연령 + 4] × 2)과 Luscombe 공식([연령 × 3] + 7)으로 체중을 추정했다.
4. 통계적 방법
몬테카를로 시뮬레이션을 통해 나이 및 성별에 따른 추정 체중이 특정 분포를 따르지 않고 무작위로 추출됐음을 확인하기 위해 히스토그램을 작성했다. Pearson의 상관분석을 이용해 추출 체중과 추정 체중간 선형적 상관관계를 분석했다. 이 과정에서 Pearson의 상관계수(r)는 -1에서 1 사이의 값을 가지며, 양수는 양의 상관관계를 의미하는 것으로 정의했다. FCM의 유용성을 평가하기 위해, FCM으로 추정한 체중이 시뮬레이션으로 추출한 체중의 10% 및 20% 이내에 존재하는 비율을 각각 제시했다.
FCM, APLS 공식, Luscombe 공식으로 추정한 체중을 몬테카를로 시뮬레이션으로 추출한 체중과 비교하기 위해, Bland-Altman 분석을 이용했다. 이 분석은 두 검사법에 의한 양적 측정치의 일치도를 그래프로 나타내는 통계적 방법으로[16], 이를 통해 시뮬레이션으로 추출한 체중과 추정 체중 사이의 일치도를 시각적으로 확인했다. Bland-Altman 분석에서 limits of agreement는 두 검사법의 평균에서 표준편차의 1.96배 떨어진 범위로, 연구자의 판단에 따라 두 검사법의 차이를 임상적으로 받아들일 수 있는 범위로 인식된다[17]. 하지만, 본 저자는 maximum allowed difference를 5 kg으로 정의했다. 시뮬레이션 및 통계분석은 R 소프트웨어 version 3.4 (R Foundation for Statistical Computing, Vienna, Austria)를 이용했다[16,18].
결과
1. 몬테카를로 시뮬레이션으로 추출한 체중의 히스토그램 및 상자그림
Fig. 1을 통해 나이 및 성별에 따른 각 9,000개의 체중이 무작위로 추출됐음을, Fig. 2를 통해 나이별 추출 체중의 범위를 각각 알 수 있다.
Histograms showing the weight of children aged 1 to 9 years extracted by the Monte Carlo simulation (A, boys; B, girls). In the normal range of weight of each group (5-95 percentile), we randomly extracted 9,000 numbers by the simulation so that they do not show a specific distribution.
Box plots of the weight of children aged 1 to 9 years extracted by the simulation (A, boys; B, girls).
2. FCM에 대한 상관분석
몬테카를로 시뮬레이션을 통해 추출한 체중과 FCM으로 추정한 체중간 유의한 양의 상관관계를 보였다(남아, r = 0.896, P < 0.001; 여아, r = 0.899, P < 0.001) (Fig. 3).
Positive correlation between the weight estimated by the finger counting method and that extracted by the simulation (A, boys; B, girls).
3. 몬테카를로 시뮬레이션으로 추출한 체중과 FCM으로 추정한 체중의 비교
남아는 FCM으로 추정한 체중의 41.4%가 시뮬레이션으로 추출한 체중의 10% 이내에, 80.5%가 20% 이내에 각각 해당했다. 그리고, 여아는 10%와 20% 이내에 각각 39.0%와 69.1%가 해당했다(Table 1).

Proportion of weights estimated using the finger counting method within 10% and 20% of weight extracted by the Monte Carlo simulation
4. 체중 추정 방법에 대한 Bland-Altman 분석
시뮬레이션으로 추출한 체중과 3가지 방법으로 추정한 체중을 Bland-Altman 분석으로 비교한 결과, 시각적으로 높은 일치도를 보였다(Table 2). 3가지 방법 모두 나이가 증가하면서 정확도가 떨어지는 경향을 보였고, 특히 7세 이상에서는 추정 체중이 추출 체중과 큰 차이를 보였다(Fig. 4). FCM으로 추정한 체중과 시뮬레이션으로 추출한 체중의 관계를 백분율의 차이로 나타낸 Appendix 1에서도, 이와 유사한 경향을 보였다.
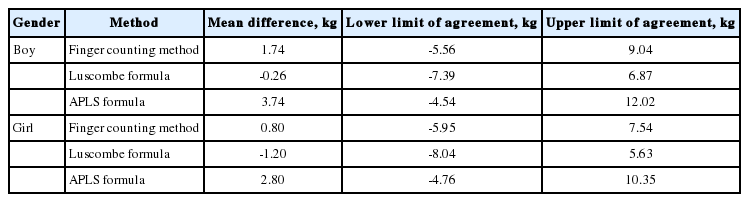
Bland-Altman statistics about the 3 pediatric weight estimation methods
Bland-Altman plots showing the 3 pediatric weight estimation methods. These plots are to compare the weight extracted by the simulation to those estimated using the finger counting method (A, D), the Luscombe formula (B, E), and the Advanced Pediatric Life Support formula (C, F). The X and Y axes represent the difference between and the average of the 2 paired quantitative measurements, respectively. Compared to the weight extracted by the simulation, the 3 methods seem to exceed the limit of agreement with the increase in age (especially in the children aged 7 years or older).
고찰
소아환자의 체중은 약물 용량과 기구 크기를 결정하는 데에 중요하지만[2], 응급상황에서는 정확한 체중을 추정하긴 어렵다. 이 어려움은 주 양육자가 아닌 보호자(예: 보육교사)의 방문 또는 의료진의 당황으로 가중될 수 있다. 최근 개발된 FCM은 응급상황에서 쉽게 체중을 추정할 수 있게 해준다[8]. 본 연구는 7세 미만의 한국 소아환자에서 FCM의 정확도가 높다는 점을 시사한다.
본 연구에서 FCM으로 추정한 체중이 무작위로 선택된 9,000개의 정상범위와 양의 상관관계를 보였다. 7세 미만 소아환자에서 FCM, APLS 공식, Luscombe 공식으로 추정한 체중은 시뮬레이션으로 추출한 체중과 높은 일치도를 보였다. 반면, 7세 이상에서는 세 공식 모두 일치도가 떨어지는 경향을 보였다. 이는 Young 등[8]이 미국 소아환자 207명을 대상으로 FCM이 다른 체중 추정 방법과 유사한 정확도를 나타내며 나이가 증가하면서 체중을 과소평가하는 경향이 있다고 발표한 것과 일치한다.
본 연구는 한국 소아환자의 인종적 특성에도 불구하고, 미국 소아를 대상으로 한 FCM의 정확도 연구[8]와 유사한 결과를 보였다. Young 등[8]이 실제 체중과 FCM으로 추정한 체중의 차이가 10%와 20% 이내에 해당하는 경우를 각각 59%와 87%로 보고했다. 이 경향은 본 연구에서 같은 범위에 포함된 비율과 유사했다. 따라서, 한국 소아환자에게서도 복잡한 공식 대신 손가락을 이용하여 간단히 체중을 추정할 수 있는 것으로 추론할 수 있다.
본 연구는 컴퓨터 시뮬레이션 연구로서 몇 가지 제한점을 가진다. 첫째, 표준성장도표를 이용했으므로, 2008년 이후 체중 변화 경향을 반영하지 못했다. 다만, 이 자료가 가장 최근 자료였다. 둘째, 1-9세의 정상범위(5-95백분위수)를 대상으로 했으므로, 연구결과를 저체중 또는 과체중 및 비만을 보이는 소아환자에게 적용하기 어렵다. 셋째, 키 또는 체형을 이용한 체중 추정 방법과 비교하지 못했다. 넷째, 본 연구에서 몬테카를로 시뮬레이션으로 추출한 체중은 특정분포를 따르지 않았으므로, 정규분포를 전제로 하는 Bland-Altman 분석에 적절치 못할 수 있다. 그런데도, 검사법 간 일치도를 시각적으로 확인하기 위해 Bland-Altman 분석을 이용했다. 향후 다양한 체중 추정 방법의 비교 외에도 임상에서 체중 추정의 소요시간 또는 사용자의 만족도를 평가하는 연구가 필요하다고 생각한다.
한국의 소아환자에서 FCM으로 추정한 체중과 몬테카를로 시뮬레이션으로 추출한 체중은 강한 양의 상관관계를 보였고, 특히 7세 미만에서 높은 일치도를 보였다. 따라서, 이 나이의 소아환자에게 FCM을 이용하여 간단하고 정확하게 체중을 추정할 수 있을 것으로 생각한다.
Notes
이해관계
본 저자는 이 논문과 관련된 이해관계가 없음.
Acknowledgements
본 저자는 이 논문과 관련된 재정지원을 받지 않았음.
References
Appendices
Appendix 1. Bland-Altman plots with differences as percentage (A, boys; B, girls).
.")