비특이적 임상증상을 나타내는 장중첩증 환자에서 응급현장초음파가 응급실 체류시간 단축에 미치는 영향
Point-of-care ultrasound may reduce emergency department length of stay in children with nonspecific manifestations of intussusception
Article information
Trans Abstract
Purpose
To investigate whether performance of point-of-care ultrasound (POCUS) can reduce emergency department length of stay (EDLOS) for children with nonspecific manifestations of intussusception (NMI), defined as 2 or less manifestations of the classic triad of intussusception, and/or vomiting.
Methods
We reviewed medical records of 141 consecutive children with intussusception aged 6 years or younger who visited the emergency department of Asan Medical Center in Seoul, Korea from May 2014 through April 2016 and underwent diagnostic radiology ultrasound and pneumatic reduction. The children were grouped according to whether they underwent POCUS or not (POCUS and no POCUS groups, respectively). POCUS was performed to children with NMI by an attending emergency physician who had completed a POCUS training course endorsed by the Korean Society of Pediatric Emergency Medicine. We measured EDLOS, which consisted of door-to-reduction and observation times. These time intervals were compared between the 2 groups.
Results
Of 112 eligible children, 65 (58%) underwent POCUS. The median EDLOS was shorter in the POCUS group than in the no POCUS group (566 minutes, interquartile range [IQR] 497 to 765 vs. 745 minutes, IQR 551 to 981; P = 0.003). The median door-to-reduction and observation times were also shorter in the POCUS group (105 vs. 138 minutes, P < 0.001 and 440 vs. 628 minutes, P = 0.008, respectively). These differences were possibly due to the performance of POCUS and the trend toward early discharge after pneumatic reduction. We found 1 child with false negative result on POCUS, but there may have been more.
Conclusion
Performance of POCUS may reduce EDLOS in children with NMI.
서 론
최근 장중첩증의 진단 및 치료의 일차선택기법으로, 초음파 및 비수술적 정복술이 각각 활용되고 있다[1,2]. 이 과정에서 영상의학과 또는 소아외과 의뢰에 많은 시간이 소요되고, 정복술 이후에도 최소 6시간의 관찰이 필요하다[3,4]. 비특이적 임상증상을 나타낸 환자의 경우, 진단 과정이 더욱 지연될 수 있다. 실제로 장중첩증의 세 증후, 즉 주기적복통 또는 보챔, 종괴, 혈변이 모두 나타나는 경우는 8%-40%이며, 비특이적 임상증상으로 인해 진단이 지연되는 경우가 최대 60%로 알려져 있다[5]. 장중첩증 진단의 지연은, 응급실 체류시간 연장을 초래할 수 있다.
응급현장초음파(point-of-care ultrasound, POCUS)는 임상의사가 현장에서 응급질환의 선별검사 및 치료를 목적으로 시행하는 초음파 검사이다[6]. 2008년 이후 POCUS 보급이 증가하면서[7,8], 응급실 체류시간 단축을 위한 방안의 하나로 제시되고 있다[9]. POCUS의 장점은 임상의사가 짧은 시간에 시행함으로써 그 결과를 진단 및 치료 계획에 즉시 반영할 수 있다는 점이다[6]. 최근 장중첩증 환자에 대해서도 POCUS를 통한 신속한 진단 가능성이 제기되고 있다[10–13]. 이는 초보자가 장중첩증 선별검사 목적으로 시행한 POCUS의 민감도와 특이도는 각각 85%, 97%였다는 보고에 의해 뒷받침될 수 있다[14]. 신속한 진단은 응급실 체류시간 단축으로 연결될 수 있다.
본 연구는, POCUS 시행이 비특이적 임상증상을 나타낸 장중첩증 환자에서 응급실 체류시간을 단축할 수 있는지 여부를 조사하기 위하여 시행되었다.
대상과 방법
1. 연구대상
본 연구는, 2014년 5월부터 2016년 4월까지 장중첩증의 가능성이 있지만 비특이적 임상증상으로 서울아산병원 소아응급실을 방문한 6세 이하 환자 중, 영상의학과 의사가 시행하는 초음파(영상의학과 초음파)를 통해 장중첩증을 진단받고 투시검사유도 공기정복술(정복술)로 치료받은 환자를 대상으로 하였다. 비특이적 임상증상은, 장중첩증의 세 증후 중 두 개 이하의 증상 또는 구토를 나타낸 경우로 정의하였다. 연구기간 동안, 연간 약 35,000명의 환자가 소아응급실을 방문하였고, 영상의학과 초음파 및 정복술이 각각 장중첩증의 진단 및 치료의 일차선택기법으로 활용되었다. 수술은 증상 지속시간이 48시간 이상이거나 장천공이 명백한 경우 또는 정복술이 2회 이상 실패한 경우에 시행되었다. 정복술 시행 후, 환자는 증상 재발 및 경구 섭취 여부에 따라 응급실에서 6–12시간 관찰 후 귀가하였다. 본원에서 장중첩증을 2회 이상 진단받은 경우에는 첫 번째 방문만을 포함하였다. 영상 진단 후 전원 된환자, 장중첩증 과거력이 있는 환자, 세증후를 모두 나타낸 환자는, POCUS 필요성이 떨어지는 경우로 판단하고연구대상에서 제외하였다. 분석에 앞서 환자 신원에 관한정보는 익명화하였다. 본 연구는 서울아산병원 임상연구심의위원회의 승인을 받고 시행하였다(IRB No. 2016–0328).
2. 자료수집
의무기록을 바탕으로 표준화된 증례 보고 양식을 이용하여, 후향적으로 환자에 대한 정보를 수집하였다. 국제질병분류 10판(International Classification of Diseases,10th revision)에 따른 장중첩증 진단코드와 본원의 정복술 술기코드를 이용하여, 환자 명단을 검색하였다.
임상적 변수로, 연령(월), 성별, 복부 수술력, 증상 지속기간, 구토, 복통(48개월 미만은 보챔), 종괴, 혈변, 복부팽만, 설사, 최근 2주 이내의 바이러스 감염 혹은 복부외상, 혈압, 심장박동수, 호흡수, 체온, 산소헤모글로빈포화도를 기록하였다. 또한 상대적으로 드문 임상증상인 창백, 기면, 경련에 대해서도 확인하였다. 실험실검사 변수로는 백혈구와 C-반응단백질 농도를 기록하였다. 초음파결과 변수로는, 영상의학과 전문의 판독을 바탕으로 병소의 위치, 병소에 포함된 창자의 두께, 림프절 수 및 액체저류, 병적 선두부위 유무에 대하여 조사하였다. 예후 변수로는 장중첩증의 중증도, 48시간 이내 재발, 수술 및 입원 건수에 관하여 기록하였다. 중증도는 경증, 중등증, 중증의 세단계로 분류하였다[2]. 하지만, 후향적연구 설계로 인하여타원 재방문 및 사망 여부에 대한 추적조사는 시행하지 못하였다. 이상의 과정에서, 결측값이 20% 이상인 변수는 분석에서 제외하였다.
3. POCUS
5명의 소아응급실 전담 전문의(전문의)가 각자의 근무시간에 비특이적 임상증상을 나타낸 환자를 대상으로 장중첩증 선별검사 목적으로, POCUS를 시행하였다. 연구기간 초기에 각 전문의의 소아 초음파 경력은 다양하였지만, POCUS 시행 전 자격요건으로, 대한소아응급의학회가 주관하는 “소아응급초음파 기초과정”을 1회 이상 이수한 경우로 하였다. 응급의학과 전문의의 자격 기준으로 초음파 150례 시행을 제시한 지침을 준용하여[15], 소아 초음파 시행 횟수가 150례 미만인 경우를 초보자, 150례 이상인 경우를 비초보자로 각각 정의하였다. 이 정의에 의하면, 전문의 중 3명이 초보자에 해당하였다. POCUS에서 전형적인 target sign 또는 pseudokidney sign이 확인된 경우를 양성으로 정의하였고, 모든 양성 환자에게 영상의학과 초음파를 시행하였다. 음성 환자는 다른 응급질환이 의심되지 않을 경우, 영상의학과 초음파를 포함한 추가 검사없이 귀가하였다. POCUS에 소요된 시간을 측정하지 못하였지만 통상 5분 이내에 완료되었고, 환자에게 추가 비용은 부과되지 않았다. 연구기간 동안, 전문의 구성은 교체 및 탈락 없이 유지되었고, 1인당 근무시간은 동일하였다. POCUS에 사용된 초음파 장비는 iE33 (Philips Ultrasound, Bothell, WA, USA)이었다.
4. 시간 변수 측정
응급실 체류시간은, 의무기록을 바탕으로, 응급실 도착으로부터 퇴실까지 소요된 시간으로 정의하였다. 퇴실 시각은 귀가 및 입원 여부와 무관하게 응급실을 떠난 시각으로 정의하였다. 추가로 응급실 체류시간을 방문-정복 시간과 관찰 시간으로 나누어 분석하였다. 방문-정복 시간은, 응급실 도착으로부터 정복술 성공까지 소요된 시간으로 정의하였다. 또한, 이 변수를 영상의학과 초음파를 통한 장중첩증 진단을 기준으로, 방문-초음파 시간과 초음파-정복 시간으로 나누어 분석하였다. 관찰 시간은 정복술 성공으로부터 퇴실까지 소요된 시간으로 정의하였다.
5. 통계적 방법
연속형 변수에 대해서는 정규분포 여부에 따라 Student t-test 또는 Mann-Whitney U test를 사용하였다. 범주형 변수에 대해서는 Chi-square test 또는 Fisher exact test를 사용하였다. 또한 초보자 여부에 따른 POCUS 시행 빈도의 차이를 Chi-square test로 분석하였다. P가 0.05 미만인 경우를 통계적 유의성이 있는 것으로 정의하였다. 시간 변수는 소수점 이하 첫째 자리에서, 그 외 변수는 둘째 자리에서 반올림한 수치를 기입하였다. 통계적 분석에는 IBM SPSS ver. 21.0 (IBM Co., Armonk, NY, USA)을 사용하였다.
결 과
연구기간 동안 정복술로 치료받은 장중첩증 환자 141명중 29명을 제외하고, 비특이적 임상증상을 나타낸 112명을 연구에 등록하였다(Fig. 1). 제외된 환자 29명 중 5명은 수술(복강경 도수정복 4건, 우측결장반절제술 1건)을시행 받았다. POCUS는 112명 중 65명(58%)에게 시행되었다. 연령의 중앙값은 18.0개월(사분위수 범위, 11.0–29.8개월)이었고, 남자 환자는 77명(69%)이었다. 가장 흔한 임상증상은 복통 또는 보챔(83%)이었고, 구토(41%)가 그 뒤를 이었으며, 증상 지속기간의 중앙값은 9시간(사분위수 범위, 4–24시간)이었다. 병소의 위치는 1건의 결장-결장 장중첩증을 제외하면, 모든 증례가 회결장 부위에서 발생하였다. 48시간 이내 재발 환자는 14명(13%)이었고, 입원 환자는 12명(11%)이었다.
Flowchart for the selection of children. POCUS: point-of-care ultrasound.
임상적 변수는 두 군 간의 차이를 보이지 않았고, 실험실검사 및 초음파결과 변수 중, C-반응단백질 농도, 액체저류는 비 POCUS군에서 빈도가 높았다(Table 1, 2). 예후 변수 4종 모두, 두 군 간의 차이를 보이지 않았다(Table 2). 수술 환자 5명을 포함하여 추가로 분석한 결과, 수술 환자 비율은 두 군 간의 차이를 보이지 않았다. 병적 선두부위가 발견된 환자는 2명으로 각각 헤노흐-쇤라인자색반증과 메켈게실이었으며, 후자에게는 정복술 성공 후 추가로 복강경 절제술이 시행되었다. 연구기간 중 확인된 사망 환자는 없었다.

Comparison of clinical features and laboratory values between the POCUS and no POCUS groups

Comparison of ultrasound results and prognosis between the POCUS and no POCUS groups
POCUS가 시행된 장중첩증 환자 65명 중 64명은 양성이었고, 모두 영상의학과 초음파를 통해 장중첩증이 확인되었다. POCUS 음성으로 귀가한 환자에 대한 추적조사는 시행하지 못하였기 때문에 전체 위음성 환자를 확인할 수 없었지만, 본 연구에서 확인된 환자는 1명이었다. 이 환자는 POCUS 음성 결과 확인 후 응급실 관찰 중 혈변이 발생하였고, 이후 시행한 영상의학과 초음파에서 장중첩증이 진단되어 정복술 시행 후 합병증 없이 귀가하였다. 연구기간 중, POCUS 시행은 증가하는 경향을 보였고(Fig. 2), 시행 빈도는 초보자에서 높게 나타났다(초보자 vs. 비초보자, 71.4% vs. 40.8%; P = 0.001).
Quarterly trend for performance of point-of-care ultrasound (POCUS) from May 2014 through April 2016 (n = 112). The performance has been increased with some degree of fluctuation during the study period. In the POCUS group, novice users performed POCUS more frequently than did non-novice users.
응급실 체류시간의 중앙값은 624분(사분위수 범위,509–832분)이었고, POCUS군 및 비 POCUS군에서 각각 566, 745분이었다(P = 0.003) (Table 3). 응급실 체류시간을 구성하는 방문-정복, 방문-초음파, 초음파-정복, 관찰 시간은 공통적으로 POCUS군에서 짧은 중앙값 및 좁은 사분위수 범위를 보였다.
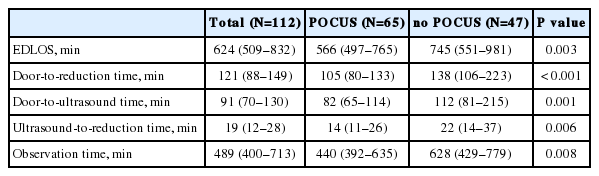
Comparison of time intervals between the POCUS and no POCUS groups
고 찰
본 연구는, 비특이적 임상증상을 나타낸 장중첩증 환자에게 POCUS를 시행할 경우 응급실 체류시간을 단축시킬수 있음을 제시한다. 응급실 체류시간의 중앙값(10시간)은, 최근 보고된 정복술 시행 환자의 응급실 체류시간 평균값(11시간)에 비하여 짧게 나타났다[4]. 응급실 체류시간을 구성하는 모든 변수가 공통적으로 POCUS군에서 짧은 중앙값과 좁은 사분위수 범위를 보였다. 이는 POCUS군에 속한 환자 중 일사분위수와 삼사분위수 사이에 속한 50%는, 비 POCUS군에 속한 환자 중 같은 기준의 50%에 비해, 비교적 신속하고 일정한 진료를 받았음을 시사한다. 특히 방문-초음파 및 방문-정복 시간은 POCUS군에서 중앙값 기준으로 각각 30분 및 33분이 단축되었고, 이는 신속한 진단 및 치료가 이루어졌음을 시사한다.
본 연구에서 보고된 장중첩증 환자의 연령, 성별, 임상증상은 최근 연구 결과와 대체로 일치한다[17–19]. 소장 장중첩증이 발견되지 않은 것은, 정복술을 시행한 환자만 포함한 것에 기인한 것으로 추정된다. 48시간 이내 재발률은최근 메타분석에서 보고된 2.7% (95% 신뢰구간, 1.2%–6.5%)에 비해 높은 경향을 보였는데[20], 이는 모든 재발 의심 환자에게 초음파를 시행한 것과 연관되었을 수 있다. 반면, 입원 및 수술 환자 비율은 기존 연구에서 보고된 입원율(18%–24%) 및 수술률(7%–23%)에 비해 낮은 경향을 보였다[4,17,19,21]. 최근 발표되고 있는 정복술 후 조기 귀가를 지지하는 연구의 영향으로[21,22], 입원율이 낮아졌을 가능성이 있다. 한편, 낮은 수술률은 본 연구에서 증상 지속기간이 기존에 보고된 19–65시간에 비해 짧았던 점에서 기인했을 수 있다[18,23].
응급실 체류시간의 단축은 POCUS 시행에 기인했을 가능성이 높다. 비록 비 POCUS군에서 C-반응단백질 농도와 액체저류의 빈도가 높았지만(Table 1, 2), 중증도를 포함한 예후 변수는 두 군 간의 차이를 보이지 않았다. POCUS 시행에 따른 방문-초음파 시간 외에도 초음파-정복 및 관찰 시간 모두 POCUS군에서 유의하게 짧았다. 연구기간 동안 정복술의 시술자, 장비, 의뢰 절차에 변화가 없었기 때문에, 이러한 요인이 초음파-정복 시간 단축에 기여했을 가능성은 낮다. 장시간 지속된 장중첩증이 병소의 부종을 초래함으로써 정복술 성공을 저해할 수 있다는 가설이 제기된 바 있다[24]. 이 가설에 의하면 신속한 진단을 초음파-정복 시간 단축의 원인으로 추정할 수 있지만, 본 연구에서는 이 기전에 대해서 분석하지는 못하였다. 연구기간 후반으로 갈수록 POCUS 시행이 증가하는 경향을 보였다(Fig. 2). 또한, 최근 보고된 정복술 후 조기귀가를 지지하는 연구가 관찰 시간 단축에 기여했을 가능성이 있다[3,4]. 따라서, 관찰 시간 단축에는 이 두 요소가 모두 영향을 미쳤을 것으로 추정된다.
POCUS 시행이 비특이적 임상증상을 나타낸 장중첩증 환자의 진단을 촉진한다는 주장은, 두 가지 근거로 뒷받침할 수 있다. 첫째, POCUS가 담낭염, 충수염, 자궁외임신, 정상임신 진단에 사용될 경우 응급실 체류시간 단축에 도움이 된다고 보고되었고[25–28], 2009년 이후 POCUS에 의한 장중첩증 조기 진단 증례가 보고되고 있다[10,13]. 둘째, 장중첩증은 상대적으로 POCUS를 통해 진단하기 쉬운 질환으로 여겨진다. 실제로, 초음파 경험이 적은 소아응급실전문의가 장중첩증 선별검사 목적으로 시행한 POCUS의 민감도와 특이도는 각각 85%와 97%로[14], 영상의학과 3년차 이하 전공의에서 보고된 결과(민감도 83%, 특이도 97%)에 근접하였다[29]. 본 연구에서는 POCUS 시행 빈도가 초보자에서 높았다. 다만 위양성률 및 위음성률을 측정하지 못하였기 때문에, POCUS의 진단가치를 평가할 수는 없었다.
장중첩증 진단에 있어서 POCUS의 중요한 단점은, 위음성 가능성이다. 초보자가 장중첩증 선별검사 목적으로 시행하는 POCUS는 특이도에 비해 낮은 민감도로 인하여[14], 음성 결과 단독으로 진단을 배제하기 어렵다. 따라서 POCUS 음성 환자에 대해서는, 검사 후 관찰 혹은 위음성 가능성에 대한 대비가 필요할 것이다. 장중첩증 선별검사를 위한 POCUS 시행에 반대하는 주장에 의하면, POCUS에서 장중첩증이 확인된 경우에도 정복술 시행에 따른 추가 비용과 시간 지연이 초래될 수 있다고 한다[30]. 본 연구에서는, POCUS 시행에 의해 진단 및 치료에 소요되는 시간이 감소한 데다가, POCUS 시행 자체에 비용을 부과하지 않았기 때문에, 상기 주장은 해당되지 않는다.
본 연구의 제한점은, 첫째, 두 군 간 맹검이 시행되지 않았기 때문에, 연구자의 개입에 의해 시간 변수가 단축되었을 가능성이 있다는 점이다. 하지만, 연구기간 중 전문의가 본 연구계획을 인지하지 못하였으므로, 그 가능성이 크다고 보기는 어렵다. 둘째, 비특이적 임상증상 외에는 일정한 POCUS 시행 기준이 미비하였기 때문에, 환자의 중증도 또는 POCUS 숙련도의 차이가 시행 빈도에 영향을 미쳤을 가능성이 있다. 하지만 두 군의 중증도에 차이가 없었던 데다가, 초보자에서 시행 빈도가 높았다. 셋째, 의무기록을 근거로 시간 변수를 측정하였기 때문에, 각 변수의 오차가 응급실 체류시간 단축에 영향을 미쳤을 가능성을 배제할 수 없다. 마지막으로, 전체 POCUS 위음성 환자 수를 확인할 수 없었다.
POCUS는 비특이적 임상증상을 나타낸 장중첩증 환자의 응급실 체류시간을 단축하는 데 기여한다. 이는 신속한 진단에 기인할 가능성이 높지만, 정복술 후 조기 귀가를 지지하는 연구의 영향일 가능성도 있다.
