열발작으로 응급실을 방문한 환자의 임상 양상
Clinical aspects of patients visiting the emergency department with febrile seizure
Article information

Trans Abstract
Purpose
We aimed to analyze the clinical characteristics, recurrence, neurological outcomes, and the impact of coronavirus disease 2019 pandemic in children who visited 2 emergency departments (EDs) with febrile seizure (FS).
Methods
We retrospectively reviewed medical records of 3,172 episodes, involving 2,510 children aged 6-60 months whose diagnoses were FSs at the EDs in 2 hospitals from 2013 through 2022. Through the review, we analyzed clinical characteristics and associated factors for the recurrence of FS. As a sub-analysis, the variables were compared between before (2017-2019) and during (2020-2022) the pandemic.
Results
A total of 3,172 FS-related visits to the EDs were found in 2,510 children. Of these, 890 children (35.5%) underwent recurrences of FS. The recurrence of FS was associated with boys (63.3% vs. 57.8%; P = 0.007), seizures lasting longer than 5 minutes (16.6% vs. 12.7%; P = 0.007), family history of FS (23.7% vs. 16.2%; P < 0.001), complex FS (13.3% vs. 8.0%; P < 0.001), and epilepsy diagnosed thereafter (9.1% vs. 3.0%; P < 0.001). During the pandemic, we noted a decrease in the number of FS-related visits to the EDs (from 1,274 to 383), an increase in the percentage of complex FS (9.3% vs. 13.8%; P = 0.012), and a decrease in the percentage of recurrent FS (49.4% vs. 33.4%; P < 0.001), compared to before the pandemic.
Conclusion
Our study identified factors associated with recurrence of FS, and confirmed the increase in complex FS with the decrease in the recurrence during the coronavirus disease 2019 pandemic. These findings could be helpful when caring for children with FS in EDs.
서론
열발작은 영유아에서 가장 흔한 발작으로, 응급실 방문의 흔한 이유이다(1-4). 열발작은 약 1/3에서 재발하며 이에 관해 연구가 많이 이뤄졌다(4). 열발작 재발은 발병 당시 나이, 열발작 가족력, 발작 지속 시간, 24시간 내 반복 발작, 발작 형태, 발병 당시 체온 등의 영향을 받을 수 있다(5-7). 열발작 환자의 신경학적 예후는 양호하며, 열 없는 발작(afebrile seizure)으로 진행하거나 신경학적 결손 또는 사망에 이르는 경우가 드물다. 그러나 뇌전증 가족력, 열발작의 잦은 재발, 비전형적 열발작은 향후 뇌전증으로 이어질 수 있다(5-7).
본 연구에서는 열발작으로 2개 병원 응급실을 방문한 소아환자의 임상 양상, 재발, 신경학적 예후, 열발작 연관 방문에 대한 코로나바이러스병-19 범유행의 영향을 분석하고자 한다.
대상과 방법
1. 연구 설계
본 연구는 후향적 의무기록 연구로 연세대학교 세브란스병원 또는 강남세브란스병원 응급실을 방문한 열발작 환자의 의무기록을 분석했다. 2013년 1월-2022년 12월 상기 2개 응급실을 방문한 6-60개월의 소아 중 열발작을 진단받은 환자를 대상으로 했다. 열발작은 응급실 방문 전 또는 체류 중 열(≥ 38 ℃)을 동반하여 발생한 발작으로 정의했다. 응급실 방문 전 뇌전증 진단, 뇌 병소, 열 없는 발작, 외상 연관 발작, 중추신경계 감염, 대사 이상 환자는 제외했다. 본 연구는 강남세브란스병원 임상연구심의위원회의 승인을 받았고, 후향적 의무기록 연구로 동의서는 면제됐다(IRB no. 3-2022-0490).
2. 연구 방법
의무기록을 바탕으로 수집한 임상적 특징은 다음과 같다. 환자의 성별, 방문 당시 나이(월), 입원 여부, 발작 지속 시간 및 양상, 열발작 가족력, 복합 열발작 여부, 열발작 시 병발(竝發) 질환을 확인했다. 과거력은 응급실 방문 당시 보호자 진술에 근거한 의무기록으로 확인했으며, 기타 항목에는 부모, 형제를 제외한 친척의 가족력까지 포함했다. 복합 열발작은 발작이 15분 이상 지속하거나, 국소 발작, 또는 발작이 24시간 이내 2회 이상 발생하는 경우로 정의했다(2,8). 임상 양상은 같은 환자가 열발작으로 2회 이상 방문한 경우를 고려하여, 환자별 분석 대신 응급실 방문 건수별 분석을 시행했다. 단, 열발작 재발 여부 및 재발과 연관된 변수 분석은 환자별로 분석했다. 열발작 재발은 열발작으로 2회 이상 방문 기록이 있거나, 첫 방문 시 열발작 과거력이 확인된 경우로 정의했다. 신경학적 예후와 관련하여, 열발작으로 방문 이후 뇌전증, 발달 지연, 자폐증, 뇌성마비 진단 여부를 확인했으며, 2022년까지 2개 병원의 의무기록을 확인했다. 추가로, 연도별, 월별 열발작 관련 방문 건수 및 코로나바이러스병-19 범유행 관련 방문 양상 변화(2017-2019 대 2020-2022)를 분석했다.
3. 통계 분석
자료 분석은 SPSS Statistics ver. 22 (IBM Corp.)를 사용했다. 각 변수의 빈도 차이는 카이제곱 검정을 사용하여 비교했으며 P < 0.05를 통계적으로 유의하다고 정의했다.
결과
열발작 연관 방문 총 3,278건 중, 방문 전 뇌전증 진단 79건, 뇌 병소 12건, 열 없는 발작 4건, 외상 연관 발작 8건, 중추신경계 감염 1건, 대사 이상 2건을 제외한 총 3,172건(2,510명)의 의무기록을 검토했다. 임상 양상은 Table 1과 같다. 남자가 더 흔하고, 나이대 중에서는 13-24개월이 가장 많았다. 열발작 가족력은 647건(20.4%)에서 확인했고, 복합 열발작은 310건(9.8%)이었다. 2,510명 중 890명(35.5%)이 열발작 재발을 경험했다. Fig. 1 및 Fig. 2를 통해, 연도별 및 월별 열발작 관련 방문 건수, 코로나바이러스병-19 범유행 관련 방문 양상 변화를 나타냈다.

Clinical characteristics of the study population (N = 3,172)
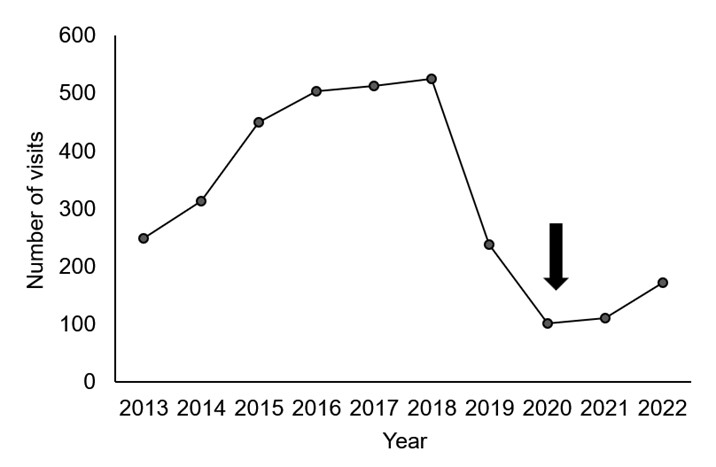
Annual trend of febrile seizure-related visits from 2013 through 2022. It shows a decrease in 2018-2020, followed by a slight rebound since the start of coronavirus disease 2019 pandemic (arrow).

Monthly trend of febrile seizure-related visits. As for the total (solid line) and during 2013-2019 (dotted line), frequent visits are noted in January and April with troughs in October. Overall decrease is noted in the visits during 2020-2022 (dash line) in comparison with 2013-2019 (dotted line).
열발작 재발은 남자, 5분 넘게 지속하는 발작, 열발작 가족력, 복합 열발작, 열발작 이후 진단된 뇌전증과 유의한 연관을 보였다(Table 2). 코로나바이러스병-19 범유행 이전 및 동안의 방문 양상을 비교한 결과, 범유행 동안 복합 열발작 빈도는 증가했고 열발작 재발은 감소했다(Table 3).

Comparisons of associated factors between the children with and without recurrence (N = 2,510)
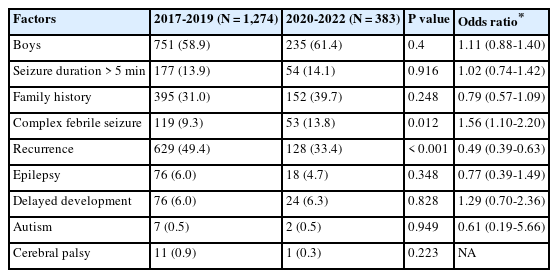
Clinical aspects of febrile seizure before and after the coronavirus disease 2019 pandemic
고찰
열발작은 12-36개월 남자가 같은 나이 여자보다 30%-100% 더 흔하게 발생하는 것으로 보고되며(8-12), 본 연구에서도 13-24개월(특히 남자)에서 호발하여 기존 연구와 일치했다. 열발작에서 유전적 소인의 연관이 추정되며 약 1/3은 가족력이 있는 것으로 알려졌다(13). 본 연구에서 가족력이 20.4%로 비교적 낮게 나온 것은 의무기록에서 가족력을 확인할 수 없거나(12.5%) 보호자가 응급실에서 가족력을 모를 경우, “없음”이라고 기록한 것에 영향을 받은 것으로 생각한다. 본 연구에서 복합 열발작의 빈도(9.8%)는 기존에 보고된 해당 빈도(25%)보다 낮다(14,15). 이는 복합 열발작의 정의 중 “24시간 이내 2회 이상 발작”을 고려하면, 귀가 직후 재발하여 외래 또는 외부 병원을 방문한 경우가 단순 열발작으로 기록될 수 있다는 점에 기인한 것으로 추정한다.
열발작 원인으로 바이러스 감염이 가장 흔한 것으로 알려진 것은 본 연구에서 상기도감염이 가장 흔하게 동반된 점과 일치한다(Table 1) (16). 코로나바이러스병-19는 12건(0.4%)이지만, 응급실 방문 당시 검사가 시행되지 않은 경우 상기도감염으로 기록된 것으로 추정된다. 열발작은 겨울에 가장 많이 발생한다고 알려진 점은(17) 본 연구에서도 확인했다(Fig. 1).
본 연구에서는 총 890명(35.5%)이 열발작의 재발을 경험했다. 재발의 위험인자로는 발열 24시간 이내, 첫 열발작을 겪은 나이가 18개월 미만, 열발작 가족력 등이 알려졌으며(5), 본 연구에서는 남자, 5분 넘게 지속하는 발작, 가족력, 복합 열발작이 유의하게 연관됐다. 발작 지속 시간이 재발과 연관되지 않았다는 기존 연구와는 차이를 보였는데(12,18), 이는 지속 시간과 발작 발생에 대한 취약성 사이의 연관을 시사하며 재발 및 뇌전증 발생에도 영향을 미치는 것으로 추정된다. 이 차이는 본 연구가 지속 시간이 비교적 긴 환자가 자주 방문하는 3차 병원 응급실에서 이뤄진 것의 영향일 수 있다. 열발작 가족력과 재발의 연관은 기존 연구와 부합한다(8,12). 복합 열발작은 재발의 위험인자로 알려졌으나(10), 일부 연구에서는 열발작 양상에 따른 재발 위험성에 차이가 없었다(6).
열발작 이후 뇌전증의 위험성에 관한 여러 연구에 따르면, 뇌전증이 열발작을 경험하지 않은 환자의 0.5%, 단순 열발작 환자의 1%-2%, 복합 열발작 환자의 6%-8%에서 각각 진단된다(19-21). 뇌전증 위험인자는 첫 열발작에 선행하는 발달장애, 뇌전증 가족력, 복합 열발작 등이다(22).
코로나바이러스병-19 범유행 동안 열발작 연관 응급실 방문은 감소했으나 복합 열발작의 빈도는 약 1.6배 증가한 반면, 재발은 약 절반으로 감소했다. 재발 감소는 범유행기에 기타 감염질환 감소, 마스크 착용, 사회적 거리두기를 통한 발열 질환의 감소로 인해 열발작 빈도가 줄어든 결과로 추정된다(23,24). 또한 이 시기에 발열 환자는 중증급성호흡증후군 코로나바이러스-2 검사 및 격리 병상 부족 등으로 3차 의료기관 방문이 제한됐다. 이에 따라 단순 열발작 환자의 응급실 방문이 감소하여, 상대적으로 복합 열발작의 수적 감소에도 불구하고 빈도는 증가한 것으로 생각한다.
본 연구의 제한점은 다음과 같다. 첫째, 의무기록의 부정확성 또는 누락이 결과에 영향을 미쳤을 수 있다. 둘째, 추적 관찰이 2개 병원에서만 이뤄졌고 범유행 동안 추적 관찰 기간이 2년 11개월 이내였으므로, 열발작 재발 및 뇌전증 발생이 과소평가됐을 수 있다. 이 점은 재발이 복합 열발작 또는 뇌전증 발생과 연관됐다는 결과에 영향을 미쳤을 수 있다. 추후 빅데이터를 활용한 전국 규모 또는 전향적 연구를 통해, 열발작의 재발 및 장기 예후를 분석해야 한다.
요약하면, 10년간 열발작으로 2개 병원 응급실을 방문한 환자에서 열발작의 재발은 남자, 5분 넘게 지속하는 발작, 열발작 가족력, 복합 열발작인 경우에 자주 발생했다. 또한, 재발한 환자에서 이후 뇌전증을 진단받은 경우가 많았다. 코로나바이러스병-19 범유행 동안 열발작 연관 응급실 방문은 감소했으나, 복합 열발작 빈도가 증가하고 열발작 재발 빈도는 감소했다.
Notes
Author contributions
Conceptualization, Resources, Software, Validation, and Visualization: Kim JM and Lee SM
Data curation: Kim JM
Formal analysis, Investigation, and Methodology: Kim JM, Hwang HY, Lee JH, and Kim MK
Project administration and Supervision: Lee SM
Writing-original draft: all authors
Writing-review and editing: all authors
All authors read and approved the final manuscript.
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
Funding sources
No funding source relevant to this article was reported.