A 14-year-old male with rhabdomyolysis associated with psychogenic polydipsia and hyponatremia
Article information

Abstract
Rhabdomyolysis associated with psychogenic polydipsia and hyponatremia is a rare condition that can cause substantial morbidity and mortality. We report a 14-year-old boy with psychogenic polydipsia who experienced recurrent hyponatremia and subsequent rhabdomyolysis. Treatment involved intravenous fluids and restriction of oral water intake. This case emphasizes the importance of early recognition and management of this condition. The possibility of rhabdomyolysis should be considered in patients with hyponatremia who have myalgia.
Introduction
Rhabdomyolysis is a potentially lethal condition characterized by rapid breakdown of the skeletal muscle tissue with leakage of toxic cellular contents into the bloodstream (1). Primary polydipsia features the excessive intake of fluids unrelated to physiological needs and the excretion of a large amount of dilute urine. It has been most commonly described in patients with psychiatric disorders with a 6%-20% prevalence, hence the frequent use of the term psychogenic polydipsia (2). Presumed etiology is dysfunction of the thirst regulation mechanism in the brain (3). Twenty-five percent of psychogenic polydipsia incurs hyponatremia, which manifests nausea, headache, lethargy, seizure, and coma (4). We report a rare case of an adolescent boy with psychogenic polydipsia presenting with recurrent episodes of hyponatremia and subsequent rhabdomyolysis. This study was approved by the institutional review board of CHA Bundang Medical Center with a waiver for informed consent (IRB no. 2023-07-053).
Case
A 14-year-old boy visited the pediatric endocrinology clinic after experiencing polydipsia, a daily water intake of 5 L/day, for over 2 weeks. The boy had a body mass index of 37.4 kg/m2 (100th percentile), a height of 176 cm (92.9th percentile), and a weight of 116 kg (100th percentile). He had a known history of attention deficit hyperactivity disorder without taking medications. Otherwise, he had been previously healthy. The patient had a family history of diabetes mellitus. The findings of laboratory tests conducted at an outside hospital, 1 week prior to the visit at our clinic, were as follows: glucose, 83 mg/dL; hemoglobin A1c, 5.5%; sodium, 125 mEq/L; and no glucose and red blood cells on the urine. At that time, no treatment was performed against hyponatremia because he did not show any symptoms.
The boy was hospitalized for evaluation of pathologic polydipsia and hyponatremia. The initial laboratory findings were as follows: sodium, 142 mEq/L; serum osmolality, 296 mOsm/kg (reference value, 275-295 mOsm/kg); urine osmolality, 484 mOsm/kg (reference value, 50-1,400 mOsm/kg, depending on volume status); and antidiuretic hormone, 1.64 pg/mL (reference value, 1-5 pg/mL). Water deprivation test was conducted to differentiate diabetes insipidus. After 6 hours, urine output and osmolality decreased to 1.3 L/kg/hour and 353 mOsm/kg, respectively. The test was terminated with the subcutaneous administration of vasopressin (2.4 units), which increased urine osmolality to 602 mOsm/kg. Sella magnetic resonance imaging showed the normal pituitary gland. Although the water deprivation test was inconclusive, both psychogenic polydipsia and central diabetes insipidus were considered given the decrease in urine output after water restriction. After discharge, the boy was found to have coronavirus disease 2019, and isolated. For this reason, he could not have a follow-up at our hospital.
Two months later, the boy presented to the emergency department (day 1) with a 4-day history of nausea, dizziness, and myalgia. The vital signs were as follows: blood pressure, 139/82 mmHg; heart rate, 71 beats/minute; respiratory rate, 18 breaths/minute; temperature, 36.1 °C; oxygen saturation, 100% in room air; and a Glasgow Coma Scale score of 14 (eye opening, 4; verbal response, 4; and motor response, 6). He did not show any seizures or focal neurological deficits. A detailed medical history revealed excessive thirst recurrence and a daily water intake > 20 L/day. A brain computed tomography was not performed given the absence of head injury and neurological deficits. Laboratory findings were as follows: sodium, 112 mEq/L; potassium, 3.6 mEq/L; chloride, 76 mEq/L; creatine kinase (CK) total, 15,042 U/L (reference value, 5-130 U/L); CK-MB fraction, 115 ng/mL; serum osmolality, 231 mOsm/kg; urine osmolality, 33 mOsm/kg; urine sodium, 4 mEq/L; aspartate aminotransferase, 287 U/L; and alanine aminotransferase, 161 U/L. Complete blood count and renal function were normal.
The boy was transferred to the intensive care unit for close monitoring of the electrolytes. Intravenous infusion of 0.9% saline was started at a rate of 150 mL/hour with water intake restricted. Fig. 1 depicts the trend of serum concentrations of CK and sodium during correction of the hyponatremia. After 6 and 12 hours of hydration, sodium concentrations were 120 and 124 mEq/L, respectively. Considering the rapid increase in sodium concentration, intravenous fluid was changed to 0.45% saline at a rate of 100 mL/hour. Six hours later, his sodium concentration increased to 132 mEq/L. Despite the rapid correction of hyponatremia, no neurological manifestations developed. The repeat CK concentration was 11,638 U/L; serum osmolality, 259 mOsm/kg; and urine osmolality, 38 mOsm/kg. The urine output was 5.2 mL/kg/hour. Thirty-six hours after hospitalization, laboratory findings were as follows: sodium, 137 mEq/L; chloride, 102 mEq/L; serum osmolality, 279 mOsm/kg; urine osmolality, 300 mOsm/kg; urine sodium, 4 mEq/L, and CK concentration, 3,738 U/L. On day 4, CK value decreased to 1,311 U/L. Urinary myoglobin concentration remained negative throughout the treatment period. Through psychiatric consultation, the boy was found to have underlying anxiety. He was advised to restrict water consumption to less than 2 L/day, and sertraline and clonazepam were prescribed to ease the anxiety disorder. Twelve months after discharge, he was doing well without another hospitalization.
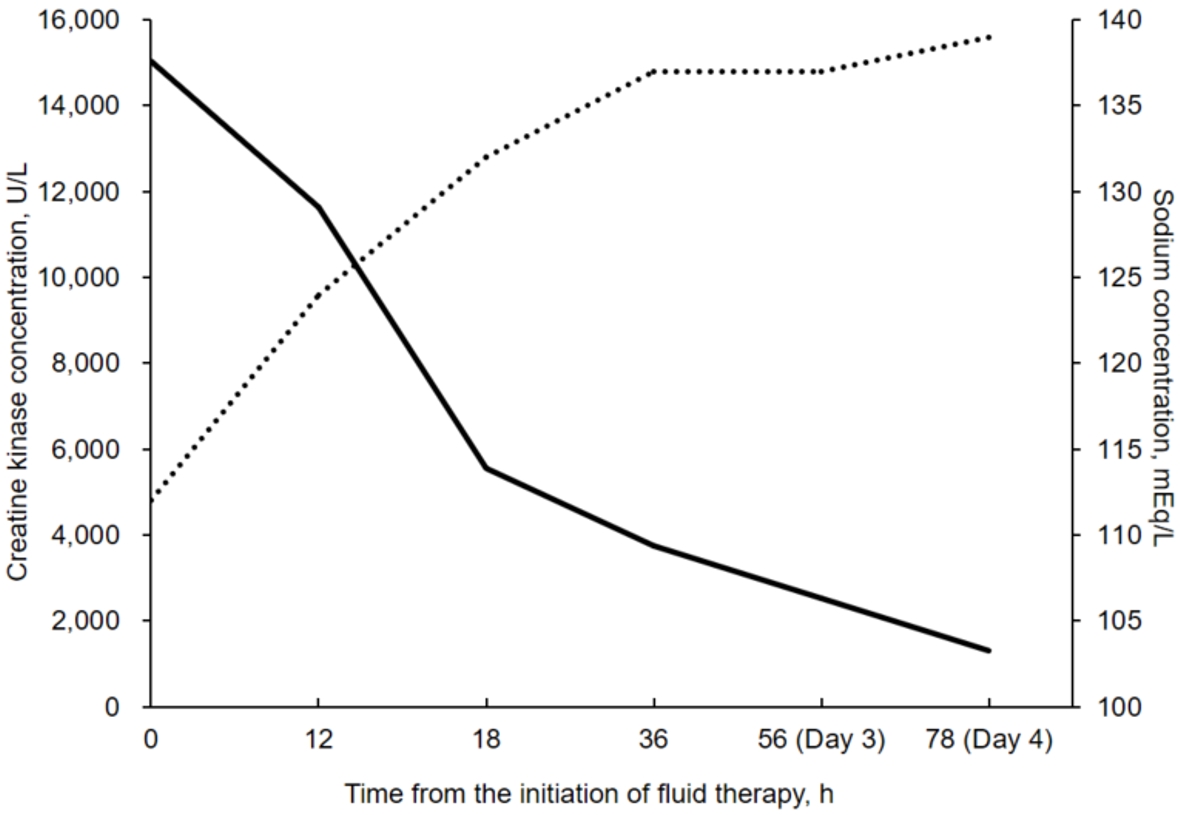
Trend of serum concentrations of creatine kinase (solid line) and sodium (dotted line) during correction of hyponatremia and development of rhabdomyolysis. The “0 hour” indicates the starting point of intravenous infusion of 0.9% saline.
Discussion
This report describes an adolescent boy who developed symptomatic hyponatremia, and subsequent rhabdomyolysis secondary to excessive water intake. The sodium concentration was corrected with 0.9% saline within 36 hours to prevent further neurological complications. A decreasing trend was noted in the CK concentration though it did not reach the normal value. The boy was discharged without any neurological or renal complications.
Common causes of rhabdomyolysis include trauma, strenuous physical activities, certain drugs and toxins, status epilepticus, sepsis, inherited muscle disorders, and electrolyte imbalances (especially hypokalemia) (5). Since 1979 when Browne (6) reported the first case of hyponatremia-induced rhabdomyolysis in a water-intoxicated, 62-year-old man, low sodium concentration has been considered another trigger of rhabdomyolysis.
Hyponatremia-induced rhabdomyolysis has been reported in only a few cases, mostly of adults with certain psychiatric conditions on antipsychotic drugs (2,4,7). The first pediatric case of rhabdomyolysis was documented in a child with influenza A (8). Recurrent rhabdomyolysis associated with polydipsia-induced hyponatremia was reported in a case series consisting of 11 adults (9). Only 1 pediatric case of this condition presents a 16-year-old boy with a known psychiatric disorder who was hospitalized with 3 consecutive episodes of severe hyponatremia and rhabdomyolysis (10). The 16-year-old boy was treated with 3% saline and supportive care, such as endotracheal intubation (10). Our case is notable in that the boy exhibited relatively mild symptoms despite the markedly low serum sodium concentration and no use of 3% saline.
There may be 3 hypotheses regarding the mechanism underlying the hyponatremia-induced rhabdomyolysis. First, as the osmolality of the extracellular fluid decreases, intracellular potassium is released from the cells, lowering the cellular transmembrane potential, which in turn causes cell destruction (2,11). Second, the rapid correction of hyponatremia can lead to inadequate cell volume regulation, potentially causing membrane fragility and enzyme leakage (13). Third, a dysfunction of the sodium-calcium pumps leads to intracellular calcium accumulation. This increased intracellular calcium activates the proteases and lipases responsible for cell lysis (2,12).
The management of rhabdomyolysis and hyponatremia requires different approaches to fluid therapy. Rhabdomyolysis must be treated with early aggressive hydration with urine alkalization to prevent acute kidney injury (5). Treatment for hyponatremia depends on its underlying cause and severity. In cases of hyponatremia in polydipsia, treatment involves fluid restriction or administration of 3% saline (10). We chose to correct the boy’s sodium concentration and preserve renal function by maintaining 0.9% saline while restricting oral water intake.
To the authors’ knowledge, this is the first Korean pediatric case of rhabdomyolysis secondary to psychogenic polydipsia and hyponatremia. We recommend checking the muscle enzymes in children or adolescents with severe hyponatremia who complain of myalgia. Such monitoring can help to timely identify and treat hyponatremia-induced rhabdomyolysis, thereby preventing further complications.
Notes
Author contributions
Conceptualization: Jung YS, Ha J, and Jung MK
Data curation, Visualization: Jung YS
Formal analysis: Jung YS and Choi Y
Investigation: Jung YS, Ha J, and Paek SH
Methodology: Jung YS, Choi Y, and Jung MK
Project administration: Jung MK
Resources: Jung YS and Paek SH
Supervision: Yoo EG and Jung MK
Validation: Choi Y and Jung MK
Writing-original draft: Jung YS
Writing-review and editing: Choi Y, Yoo EG, Paek SH, and Jung MK
All authors read and approved the final manuscript.
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
Funding sources
No funding source relevant to this article was reported.