전국 신체계측 조사 자료를 이용한 한국 소아의 Broselow tape 타당도 평가: 단면 연구
Validation of the Broselow tape in Korean children using data from a nationwide anthropometric survey: a cross-sectional study
Article information

Trans Abstract
Purpose
In Korea, the Broselow tape (BT) is widely used to estimate weight in resuscitation. Validation of BT in Korean children is essential because the tool was developed based on children’s weight and height in the United States. The validation was previously performed in a small-scale dataset. The authors aimed to validate BT using the 2005 Korean nationwide anthropometric survey data.
Methods
From the population used for the survey, we sampled children aged 0-12 years. The weights estimated by BT were compared with measured weights of the children using Bland-Altman analysis with results recorded as percentage differences. We measured the accuracy of BT, defined as within a 10% error of the measured weight, and the concordance of the color-coded zones derived from the estimated and measured weights. The accuracy and concordance were further assessed according to the age groups and body mass index-for-age Z-score (< -2, underweight; > 2, overweight or obese).
Results
A total of 108,128 children were enrolled. The mean age was 55.2 ± 37.5 months. The bias was –5.4% (P < 0.001), and the limits of agreement were –28.3% and 17.6%, respectively. The accuracy and concordance of BT were 64.4% and 67.2%, respectively. Differences of no more than 1 color-coded zone between estimated and measured weights accounted for 89.8% and 84.1% of the under- and overweight (or obese) children, respectively.
Conclusion
BT accurately estimates weight in approximately two-thirds of Korean children. In addition, adjustment of 1 color-coded zone may be considered in children with extreme weight.
Introduction
In children, a weight determines drug dose and instrument size. Thus, it is essential to estimate weight in resuscitation of critically ill children. The Broselow tape (BT) is a weight estimation method based on height-weight correlations [1-5]. BT was developed based on the 50th percentile of children’s weight and height in the United States, and validated using data from the population [4,6]. Given a wide use of BT outside the U.S., several validations have been conducted in other countries [7-12]. Although a Korean validation study showed a good agreement with the measured weights, the study had a high probability of bias due to the inclusion of only 665 children at a single center [13].
In 2005, the Korean Pediatric Society performed a nationwide anthropometric survey to develop the 2007 Korean National Growth Charts [14]. This was the most recent nationwide survey to measure actual body sizes of children and adolescents. In this large-scale survey, trained teams measured the sizes using a uniform method in the children and adolescents who were sampled across the country and stratified by age and region. The teams surveyed more than 4,000 children from each age younger than 13 years. Hence, the nationwide anthropometric data are likely to be representative of Korean children’s weight and height. Using the data, the authors aimed to validate the weight estimation by BT in Korean children.
Methods
1. Study design, setting, and population
This study is a retrospective, cross-sectional, secondary analysis using the above-mentioned nationwide dataset, which involved approximately 142,000 children and adolescents [14]. From the population, children aged 0-12 years were included in the current study. Data were excluded from the analysis (1) if there were missing values for the study variables (see Data extraction and study procedure section), or (2) if a height was outside the BT-applicable length (< 46.0 or > 146.7 cm).
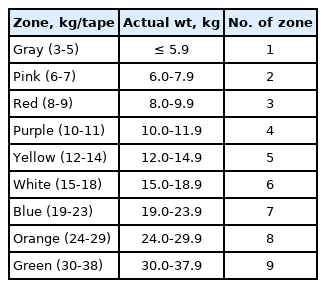
We used 2005A version BT (designated as BT from here unless otherwise specified; Armstrong Medical Inc., Lincolnshire, IL), which was used in 2005, and measured the length of the color-coded zones of the tape using a steel ruler (Komelon Corp., Busan, Korea). Although a newer version of the tool was released, we applied the version to validate its performance against the data obtained in 2005.
This study, which complies with the Declaration of Helsinki, was approved by the institutional review board of Seoul National University Hospital (IRB no. 1204-014-403), which waived the requirement for informed consent.
2. Study protocol and data analysis
1) Data extraction and study procedure
We extracted data, including sex, date of birth, date of measurement, weight (kg), and height (cm) of the study population. Age was calculated as the difference between the date of measurement and that of birth. The weights and color-coded zones were estimated by applying the measured heights to the corresponding interval of BT.
The study population was divided into the 4 age groups: infants, 0-12 months; toddlers, 13-36 months; preschoolers, 37-60 months; and schoolers, > 60 months. Among these groups, we compared the accuracy of weight estimation and the concordance of color-coded zones.
The Z-scores for body mass index (BMI)-for-age (i.e., BMI Z-scores) were calculated to examine the effectiveness of BT for children with extreme weight. BMI Z-scores of < -2.0 and of > 2.0 were considered under- and overweight (or obese), respectively. We compared the degree of discrepancy between the zones by estimated weights and those by the measured weights among the children with extreme weight. The BMI Z-scores were calculated using the 2006 World Health Organization Growth Standards for children aged 1-60 months and the 2000 U.S. Centers for Disease Control Growth Reference for those aged 61 months-12 years [15,16].
2) Outcome
The primary outcomes were (1) the accuracy of BT weight estimates, defined as within a 10% error of the measured weight, and (2) the concordance of the color-coded zones derived from the estimated and measured weights.
3) Primary data analysis
The difference and precision of the weights estimated using BT were evaluated by calculating the mean percentage error (MPE) and root mean square error. To evaluate bias and variability, the authors performed the Bland-Altman analysis as a percentage of the difference to determine the agreement limits between estimated and measured weights. We showed a percentage difference rather than an absolute value to avoid bias caused by the latter value, which inevitably goes up with increasing weight [17]. The overall accuracy of BT was determined by calculating the percentage difference of the weight estimations within 10% and 20% of the measured weight. Additionally, we compared the color-coded zones determined from estimated and measured weights. We numbered each color-coded zone and calculated the concordance between the color-coded zones of the estimated and measured weights (Appendix 1). Statistical analyses were performed using SPSS ver. 16.0 (SPSS Inc., Chicago, IL) and Stata/SE ver. 14.2 (StataCorp LLC, College Station, TX). Statistical significance was set at P < 0.05.
Results
Of the 119,157 eligible children, 108,128 were analyzed in the study (Fig. 1). The mean age was 55.2 ± 37.5 months, and 57,617 (53.3%) were boys. Their weights ranged from 2.3 to 79.2 kg. Table 1 shows the baseline characteristics of the population.
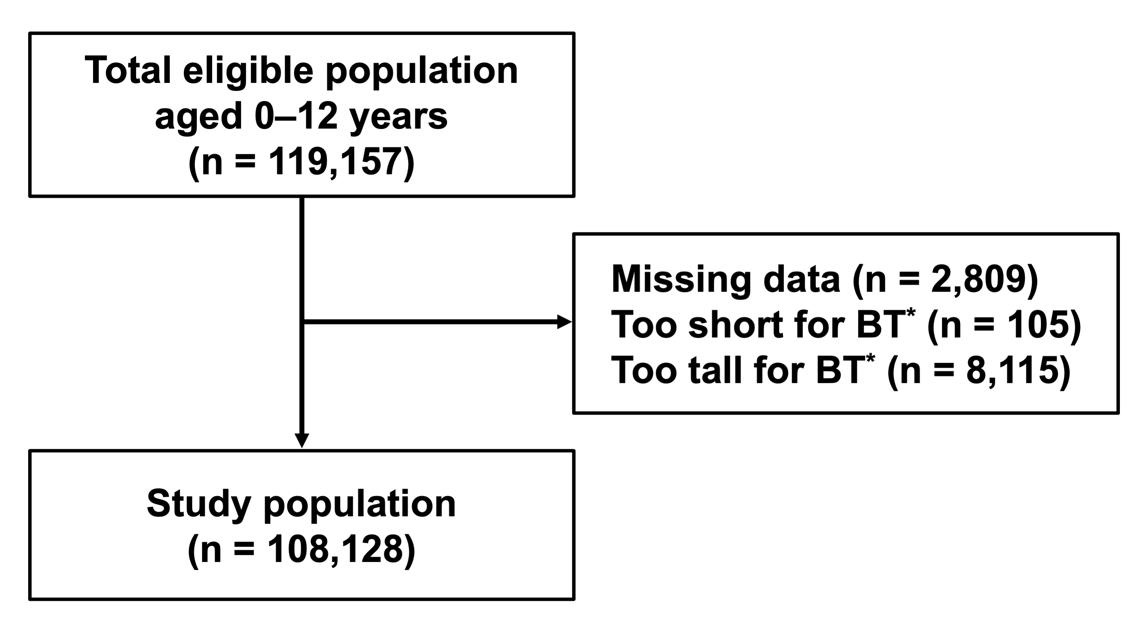
Flowchart for the selection of study population. *A height outside the BT-applicable length (< 46.0 or > 146.7 cm). BT: Broselow tape.

Baseline characteristics of the study population
According to the Bland-Altman analysis in all age groups, the bias was –5.4% (95% confidence interval, –5.4% to –5.3%, P < 0.001), and the limits of agreement were –28.3% and 17.6%, respectively (Fig. 2). These findings indicate that an estimated weight using BT was 5.4% lower than the mean measured weight. Approximately 95% of the differences between the estimated and measured weights were between –28.3% and 17.6%.
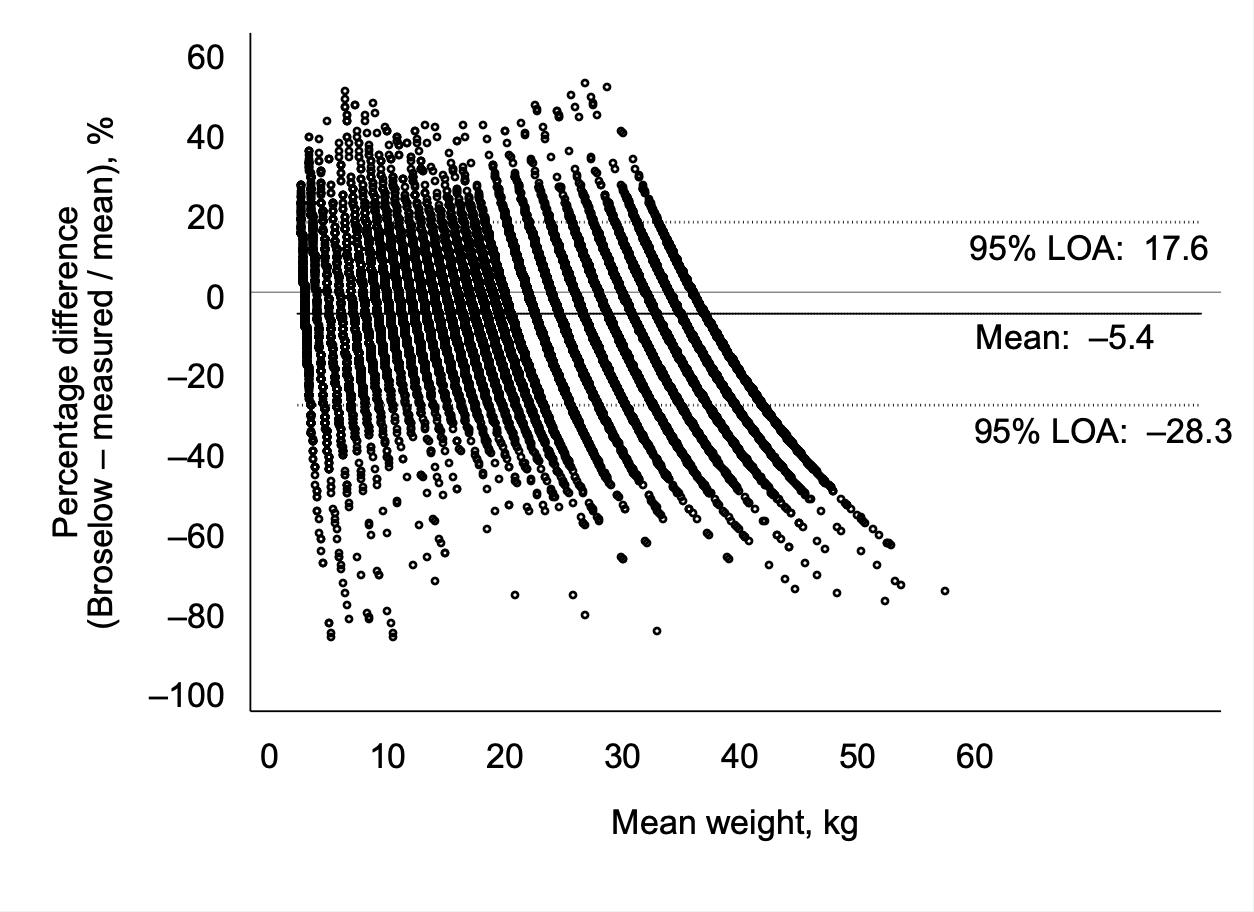
Bland-Altman plot indicating the percentages of differences showing the agreement between the estimated and measured weights. LOA: limits of agreement.
Overall, the MPE was –4.6%. The MPE showed the lowest value in the schoolers and the highest value in the toddlers. In 64.4% of the children, the difference in estimated weights was within 10% of the measured weights. The accuracy was lowest and highest in the infants (56.4%; 55.7-57.1) and the preschoolers (72.0%; 71.5-72.6), respectively. The degrees of under- and overestimation of weights according to the age groups are presented in Table 2.

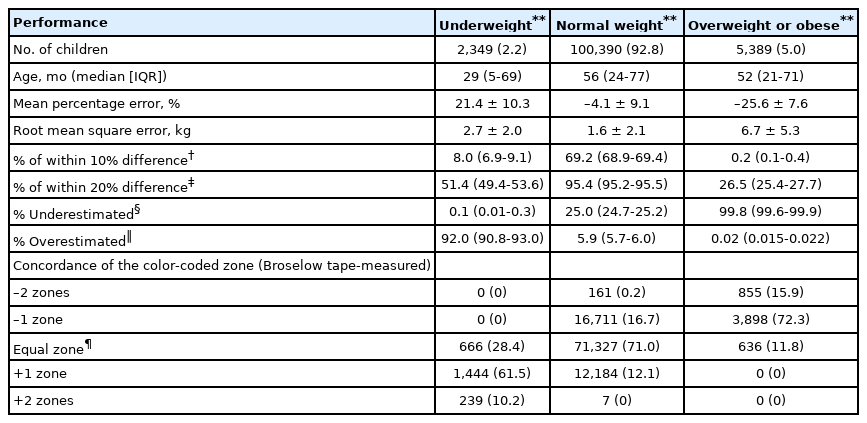
Performance of the Broselow tape
The concordance of color-coded zones was 67.2% in all age groups (Fig. 3). The infants showed the highest concordance (76.3%) while the schoolers showed the lowest rate. Measurements for which the –1 to 1 difference of the zones accounted for 98.8% across all age groups. No children differed by more than 2 zones.
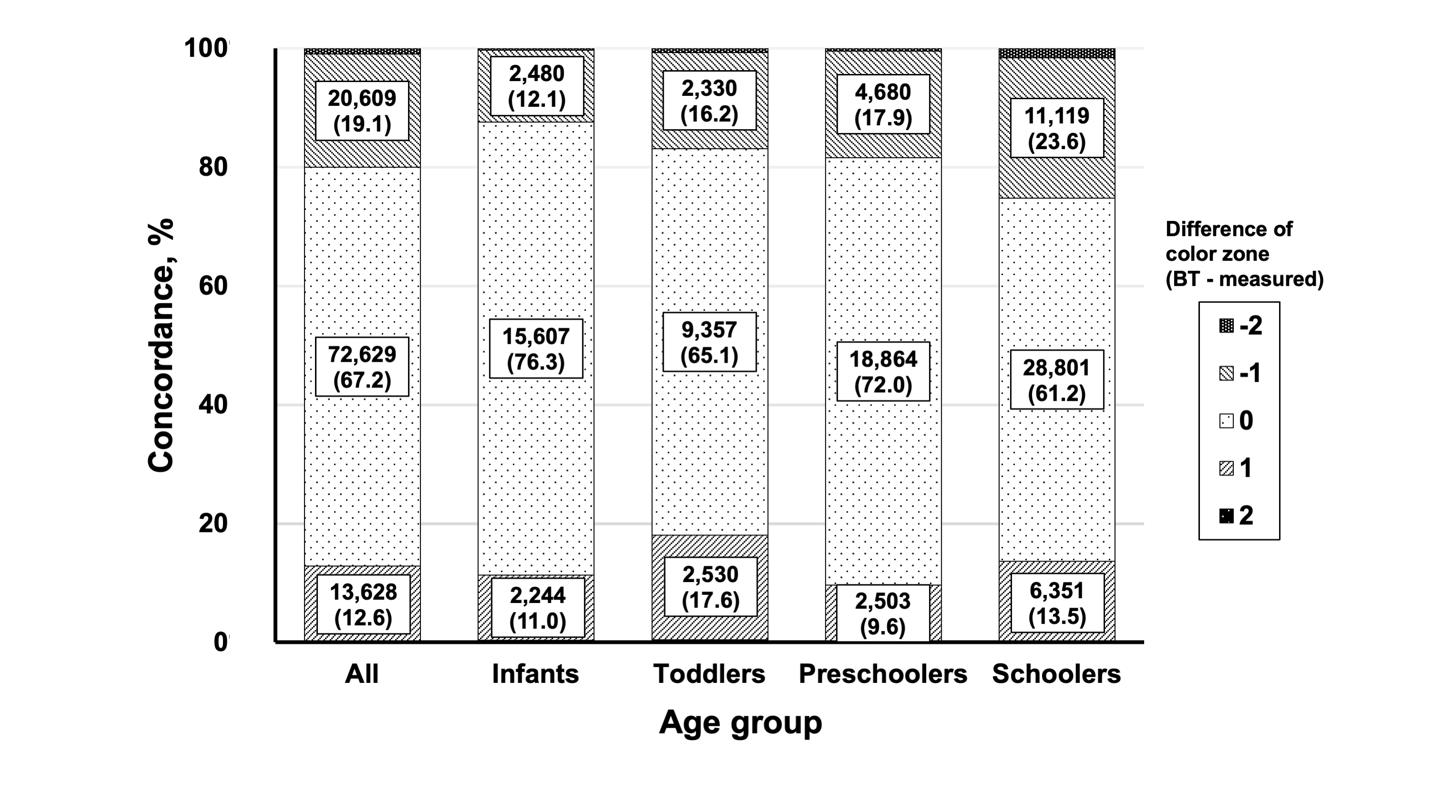
Age group characteristics of the concordance between the estimated and measured color-coded zones. BT: Broselow tape.
Table 3 shows the performance of BT in the children with extreme weight. Only 2.2% and 5.0% were considered under- and overweight (or obese), respectively. The percentages that the estimated weights differed from the measured weights by within 20% were 51.4% of the underweight children and 26.5% of the overweight children. In 61.5% of the underweight children, the color-coded zones by the estimated weights were 1 zone heavier than those by the measured weights. In 72.3% of the overweight children, the zones by the estimated weights were 1 zone lighter than those by the measured weights. Differences of –1 to 1 zone between the estimated and measured ones accounted for 89.8% and 84.1% in the under- and overweight children, respectively.
Discussion
Unlike the previous smaller-scale validations [7-12], this current study to validate BT was based on the Korean nationwide anthropometric dataset. This dataset was made by trained teams’ measurement of body sizes of children and adolescents who were sampled across the country and stratified by age and region. Thus, the study finding represents the actual performance of BT in Korean children.
A U.S. study showed an inaccurate weight estimation by the BT color-code system in one-third of the study population [7], giving a 66.2% concordance rate of the color-coded zones. Another study showed that the mean weight estimated by BT was 1.54 kg lighter than the measured weight while the accuracy of weight prediction within a 10% error was 57.9% [13]. In our study, the accuracy (64.4%) and concordance (67.2%) of BT approximate to those of the previous 2 studies. This finding suggests that BT accurately estimates weight in about two-thirds of Korean children.
As shown in Fig. 3, the concordance of color-coded zones was highest in the infants (76.3%), but their accuracy of weight estimation was only 56.4%. Considering the lighter weights of infants, the range of 10% error was narrower than those of older children. In contrast, the range of weights matched to the color-coded zones is wider than the range of 10% error, making the zones easy to match with infants’ weights. Thus, a gap could occur between the estimated weights and zones. Because drug dose and instrument size are determined by the zones in a clinical setting, the concordance of the zones may be more important than the accuracy of weight estimation itself. From this viewpoint, the highest concordance of the zones in the infants may be meaningful despite their lowest accuracy. In contrast, the toddlers showed a 70.5% accuracy with a relatively low concordance of the zones (65.1%), making BT less suitable than in the infants. Further research and development of a new resuscitation tape are required to prevent the possible discrepancies.
Our data show a lower performance of BT in the children with extreme weight. As per the instructions from the manufacturer of BT, 1 color-coded zone adjustment can be considered if a child appears overweight. Several recently developed weight estimation methods have been designed to consider the body habitus or upper arm circumference to calibrate this point. These methods have better accuracy than BT, especially in children with extreme weight [6,18,19]. However, the methods require special measuring tools and are currently used less extensively than BT. The tools are still unavailable in many countries. To compensate for this drawback, Wells et al. [20] studied the performance of a modified BT using a visual assessment of the body habitus without using any special tools, showing a better accuracy. It is required to further validate the above-mentioned weight estimation methods and adjustment of the color-coded zones by impression of body habitus in consideration of Korean children’s obesity.
This study has some limitations. First, BT was not directly applied to the children. The examiners and subject factor errors that may occur when applying BT in a clinical setting were not considered. However, this flaw may not be critical because our methods were similar to the developing process of BT [4]. Second, the 2005 dataset might not accurately reflect the contemporary body habitus. However, the developing process of BT had been unchanged from 2005 through 2019. Thus, we validated the performance of 2005A version, which was used at the time of anthropometric measurement, to indirectly evaluate the performance of a recent version of BT.
In conclusion, BT accurately estimates weight in approximately two-thirds of Korean children. Also, another two-thirds of those with extreme weight show 1 difference of the color-coded zone, suggesting the need for adjustment of 1 zone in the children.
Notes
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
Acknowledgements
No funding source relevant to this article was reported.