급성 심근염으로 인한 전신강직발작 증례
A case of generalized tonic seizures related to acute myocarditis
Article information

Trans Abstract
It is challenging to clinically distinguish between convulsive syncope and true seizure. We describe a 7-year-old girl presenting with generalized tonic seizure caused by acquired complete atrioventricular block related to acute myocarditis. After hospitalization following 6 episodes of new-onset fever with seizure, she had a short episode of abrupt complete atrioventricular block followed by another generalized tonic seizure. The concentrations of cardiac enzymes were elevated, and her echocardiogram showed a decreased left ventricular function. This case underlines the necessity of cardiac investigations in children with convulsive syncope.
Introduction
Patients with acute myocarditis may experience sudden unconsciousness with involuntary movement due to generalized cerebral hypoperfusion of cardiac etiology, which can be misdiagnosed as a true seizure. Convulsive syncope, which is a syncope accompanied by involuntary movements, differs in clinical implications from seizure. It is challenging to clinically distinguish between convulsive syncope and seizure. Without initial suspicion of cardiac etiology, there is often a diagnostic or therapeutic delay. We describe a 7-year-old girl presenting with seizure, which turned out to be convulsive syncope, caused by acquired complete atrioventricular (AV) block related to acute myocarditis.
Case
A previously healthy, 7-year-old girl presented to the emergency department with 6 episodes of generalized tonic seizures, each of which had lasted for a few seconds. There was no evidence of tongue biting or postictal confusion. Two days before the episodes, she developed an influenza-like illness comprising fever, rhinorrhea, and cough. She had no family history of cardiac or neurological diseases.
Initial vital signs were as follows: blood pressure, 137/74 mmHg; heart rate, 90 beats/min; respiratory rate, 20 breaths/min; temperature, 38.0℃; and oxygen saturation, 100% on room air. There were good peripheral pulses with capillary refill less than 2 seconds. Her heart sounds were normal without cardiac murmurs and lung sounds were clear. She had no hepatomegaly or edema. The girl was alert and responsive, and no abnormalities were detected on neurological examination.
Initial laboratory findings including blood gas analysis were all within normal limits, except aspartate aminotransferase of 68 mg/dL. The white blood cell count was 9.2 × 103/uL and C-reactive protein concentration was 0.5 mg/dL. Chest radiograph showed a cardiothoracic ratio of 0.58 on posterior-anterior view, and brain computed tomography findings were normal. No cardiac investigations were performed because she was presumed to have a seizure related to viral infection.
On hospitalization, she complained of vomiting and experienced a short episode of abrupt slowing of ventricular rate to 34 beats/min as she turned pale. Her blood pressure dropped to 80/50 mmHg. The electrocardiogram (ECG) showed complete AV block (Fig. 1A), which was followed shortly by a generalized tonic seizure lasting for 5 seconds or shorter without auras. During this episode, we noted a generalized tonic posture with the arms forcibly flexed, which was similar to previous seizures. Her blood pressure increased to 105/66 mmHg, and her consciousness rapidly recovered. Three minutes later, the following ECG showed sinus tachycardia with right bundle branch block and left anterior fascicular block (Fig. 1B). The concentrations of cardiac enzymes were as follows: creatine kinase-myocardial band fraction, 33 mg/mL (reference value, < 6.6 ng/mL); and troponin I, 0.58 ng/mL (reference value, < 0.1 ng/mL). She was transferred to a tertiary-care pediatric intensive care unit while given infusion of intravenous isoproterenol and dopamine.
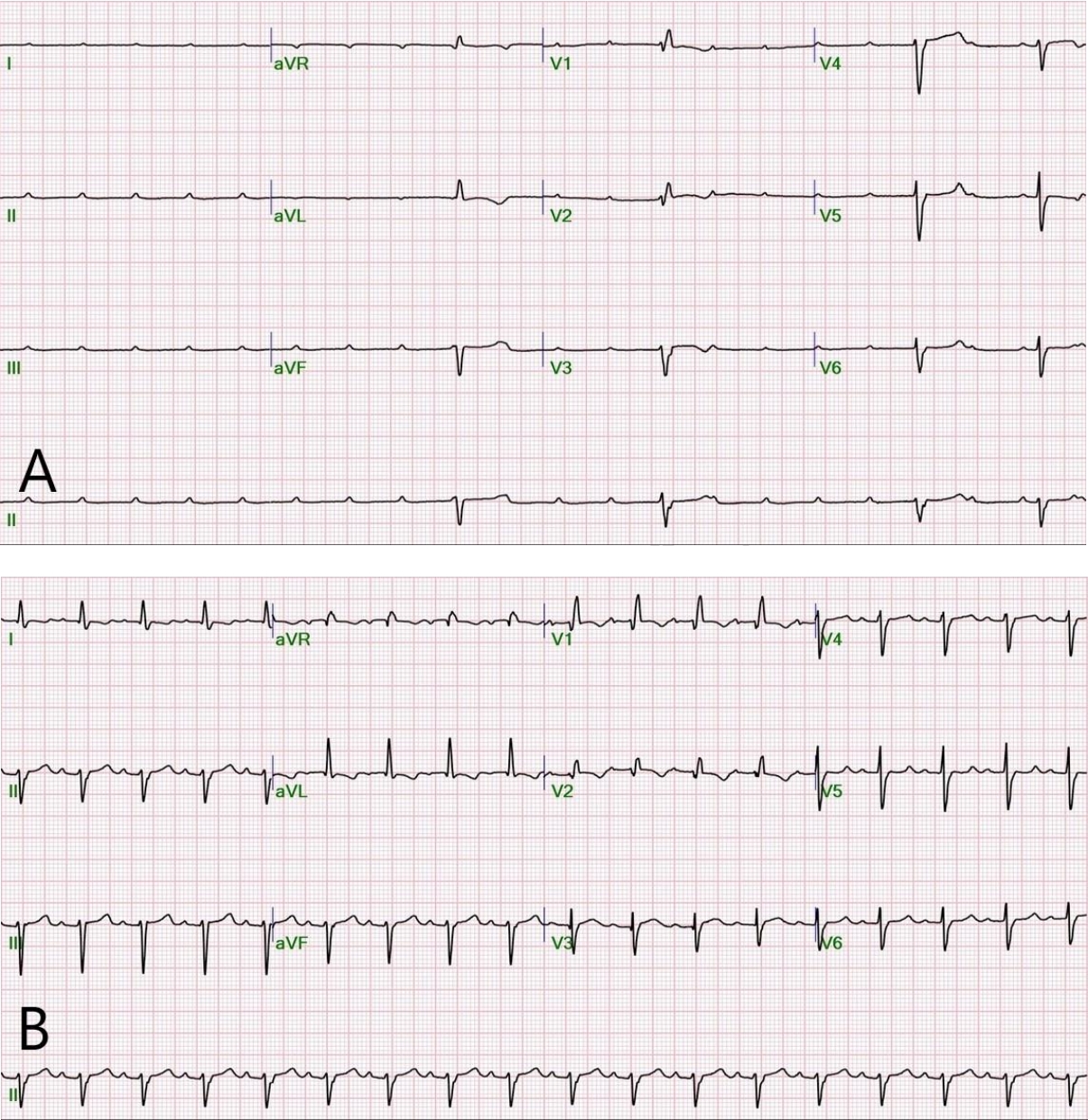
Electrocardiograms (ECGs) before and after convulsive syncope. Initial ECG (A) shows complete atrioventricular block before generalized tonic seizure (ventricular rate, 34 beats/min). Follow-up ECG (B) shows right bundle branch block and left anterior fascicular block after the seizure (ventricular rate, 106 beats/min).
After the transfer, isoproterenol was discontinued. Instead, dopamine (5 μg/kg/min) and dobutamine (10 μg/kg/min) were infused without a recurrence of AV block. Echocardiogram showed decreased left ventricular function (ejection fraction, 40%) with paradoxical wall motion and a small amount of pericardial effusion. Concentration of troponin I increased to 4.20 ng/mL. We noted the negative findings of anti-streptolysin O and anti-cytomegalovirus immunoglobulin (Ig) M, anti-herpes simplex virus IgM, anti-Epstein-Barr virus IgM, and polymerase chain reactions for human herpesvirus 6, enterovirus, and parvovirus B19. Antinuclear, anti-double stranded DNA, anti-ribonucleoprotein, anti-Sm, and anti-Ro antibodies were also negative. Her electroencephalogram showed normal findings. Based on clinical and laboratory findings, she was diagnosed with probable acute myocarditis due to unknown viral infection.
She received hemodynamic support with inotropic agents and furosemide. She was also administered intravenous Ig (2 g/kg) with antibiotics, and closely monitored over the following 72 hours. On day 4, intravenous dopamine and dobutamine were discontinued. At that time, concentration of troponin I was 1.10 ng/mL and a follow-up echocardiogram showed an ejection fraction of 55% without a pericardial effusion. The girl was discharged uneventfully on day 8. Six months later, she was fully recovered without any recurring cardiovascular symptoms or abnormal electrocardiographic findings.
Discussion
We report a 7-year-old girl with complete AV block related to acute myocarditis presenting with seizure.
Syncope caused by asystole with intermittent AV block can incur cardiogenic shock that occurred in the case patient. This phenomenon manifests as an episode of collapse associated with loss of consciousness lasting for a few seconds without a warning sign. A prolonged attack may be followed by stiffening or jerking movements[1]. A small case series suggested hypotension and convulsive seizure as additional specific manifestations of myocarditis with complete AV block[2]. Although the myocarditis-associated bradyarrhythmia can be life-threatening, the long-term prognosis is good if detected early and managed properly.
Unlike vasovagal syncope, cardiac syncope may occur without prodromal symptoms or briefly present with dizziness or palpitations[1]. This syncope can result in brief involuntary movements after pallor and loss of consciousness, mimicking a generalized tonic-clonic seizure[3]. The mechanism, by which convulsive syncope produces myotonic activity, is believed to involve the reticular formation, which has multiple inputs responsible for controlling posture, tone, balance, and auditory and visual signals to the cerebellum[4,5]. Although convulsive syncope is seemingly similar to seizure, the key aspects to clinically distinguish convulsive syncope from seizure are pallor associated with autonomic symptoms, shorter duration of abnormal movements, and recovery lasting for a few seconds. Thus, for the clinical differentiation, it is essential to obtain medical history on the collapse events from witnesses. Because cardiac syncope can mimic seizure, cardiac investigation, such as ECG, is warranted in children presenting with convulsive syncope.
It is clinically difficult to distinguish between convulsive syncope and seizure, which are common causes of visits to emergency departments or hospitalization. This case highlights the necessity of cardiac investigations in children with convulsive syncope.
Notes
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
Acknowledgements
No funding source relevant to this article was reported.