žĄú Ž°†
ÍįÄžôÄžā¨Ūā§Ž≥ĎžĚÄ žÜĆžēĄžóźžĄú ŪĚĒŪēú ͳȞĄĪ ž†Ąžč† ŪėąÍīÄžóľžúľŽ°ú, žč¨žě•Ūē©Ž≥Ďž¶ĚžĚĄ žú†ŽįúŪē† žąė žěąŽč§[1]. Intravenous immunoglobulin (IVIG)žĚĄ ž†Āžčúžóź Ūą¨žó¨Ūē®žúľŽ°úžć® žč¨žě•Ūē©Ž≥Ďž¶Ě ŽįúžÉ̞̥ žėąŽį©Ūē† žąė žěąžúľŽĮÄŽ°ú, žĚĎͳȞ觞󟞥ú ž°įÍłį žßĄŽč®ŪēėŽäĒ Í≤ÉžĚī ž§ĎžöĒŪēėŽč§[2,3]. ŪēėžßÄŽßĆ ŽĻĄŪäĻžĚīž†Ā ž¶ĚžÉĀžĚĄ ÍįĞߥ ŪôėžěźžĚė žěĄžÉĀž†Ā žßĄŽč®žĚÄ žĖīŽ†ĶÍ≥†[1], žĚīŽ°ú žĚłŪēī žßĄŽč®žĚī žßÄžóįŽźėŽ©ī žĻėŽ™Öž†ĀžĚł žč¨žě•Ūē©Ž≥Ďž¶ĚžúľŽ°ú žĚīžĖīžßą žąė žěąŽč§. žĚī ŪôėžěźÍĶįžóźžĄú Žč§žĖĎŪēú ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßą Í≤Äžā¨Ž•ľ žßĄŽč®žóź Ž≥īž°įž†ĀžúľŽ°ú žĚīžö©Ūē† žąė žěąŽč§[4]. žĚīžôÄ ÍīÄŽ†®Ūēėžó¨, ÍłįŪÉÄ žóī ÍīÄŽ†® žßąŪôė ŽėźŽäĒ žßĄŽč® žßÄžóį ŪôėžěźžôÄ Í≤Äžā¨ Í≤įÍ≥ľ ŽĻĄÍĶź, ŽėźŽäĒ Ūē©Ž≥Ďž¶Ě ŽįŹ IVIG Ž∂ąžĚĎžĄĪžĚĄ žėąžł°ŪēėÍłį žúĄŪēú Í≤Äžā¨ Í≤įÍ≥ľ ŽďĪžóź ÍīÄŪēú Žč§žĖĎŪēú žóįÍĶ¨ÍįÄ Ž≥īÍ≥†ŽźźŽč§[5-9].
ÍįÄžôÄžā¨Ūā§Ž≥ĎžĚÄ ŪėąÍīÄžóľžĚīŽĮÄŽ°ú ͳȞĄĪÍłįžóź ŽįĪŪėąÍĶ¨ žąė, C-ŽįėžĚώ讎įĪžßą ŽÜ掏Ą, ž†ĀŪėąÍĶ¨žĻ®ÍįēžÜ掏ĄÍįÄ ž¶ĚÍįÄŪēėŽ©į, žĻėŽ£Ć žĚīŪõĄ žĚľž†ē žčúÍįĄžĚī žßÄŽāėŽ©ī ž†ēžÉĀŪôĒŪēúŽč§[10]. ŽėźŪēú, Ž¶ľŪĒĄÍĶ¨, ŪėłžāįÍĶ¨, N-terminal pro-brain natriuretic peptide (NT-proBNP) žąėžĻėŽŹĄ Í≤ĹÍ≥ľžóź ŽĒįŽĚľ Ž≥ÄŪē† žąė žěąŽč§[11,12]. ͳȞĄĪÍłį Ūôėžěź ž§Ď žĚľŽ∂ÄŽäĒ ÍįÄžôÄžā¨Ūā§Ž≥Ϟ̥ žčúžā¨ŪēėŽäĒ žěĄžÉĀž¶ĚžÉĀžĚī ž°įÍłįžóź ŽāėŪÉÄŽāė Žįúžóī 5žĚľ žĚīž†Ąžóź Žį©Ž¨łŪēėÍłįŽŹĄ ŪēúŽč§. ÍįÄžôÄžā¨Ūā§Ž≥Ď Í≤ĹÍ≥ľžóź ŽĒįŽ•ł ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßą žąėžĻėžĚė Ž≥ÄŪôĒÍįÄ ŽöúŽ†∑ŪēėžßÄŽßĆ, žóī žßÄžÜćÍłįÍįĄ ŽįŹ žĪĄŪėą žčúÍłįžóź žīąž†źžĚĄ Žßěž∂ė žóįÍĶ¨ŽäĒ Ž∂Äž°ĪŪēėžó¨[5-9], Íłįž°ī žóįÍĶ¨ Í≤įÍ≥ľŽ•ľ Žįúžóī 5žĚľ žĚīž†Ąžóź Žį©Ž¨łŪēú ŪôėžěźžóźÍ≤Ć ž†Āžö©ŪēėÍłįŽäĒ žĖīŽ†§žöī žč§ž†ēžĚīŽč§. Žįúžóī 5žĚľ žĚīž†Ąžóź Žį©Ž¨łŪēú ÍįÄžôÄžā¨Ūā§Ž≥Ď ŪôėžěźžóźžĄú NT-proBNPÍįÄ žßĄŽč®žóź žú†žö©ŪēėŽč§ŽäĒ žóįÍĶ¨žóźžĄúŽŹĄ, ŪēīŽčĻ Í≤Äžā¨Í≤įÍ≥ľŽ•ľ Žįúžóī 5žĚľ žĚīŪõĄžóź Žį©Ž¨łŪēú ŪôėžěźžĚė Í≤įÍ≥ľžôÄ ŽĻĄÍĶźŪēėžßĄ Ž™ĽŪĖąŽč§[13].
žĚīžóź Ž≥ł žóįÍĶ¨ŽäĒ Žįúžóī 5žĚľ žĚīž†Ą ŽįŹ žĚīŪõĄžóź žĚĎͳȞ觞̥ Žį©Ž¨łŪēú ÍįÄžôÄžā¨Ūā§Ž≥Ď ŪôėžěźžĚė ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßą žąėžĻėŽ•ľ ŽĻĄÍĶźŪēėÍ≥†žěź žąėŪĖČŪĖąŽč§.
ŽĆÄžÉĀÍ≥ľ Žį©Ž≤ē
Ž≥ł žóįÍĶ¨ŽäĒ 2012ŽÖĄ 3žõĒŽ∂ÄŪĄį 2018ŽÖĄ 2žõĒÍĻĆžßÄ Í≤ĹžÉĀŽĆÄŪēôÍĶźŽ≥Ďžõź žĚĎͳȞ觞̥ Žį©Ž¨łŪēú 15žĄł žĚīŪēėžĚė ÍįÄžôÄžā¨Ūā§Ž≥Ď Ūôėžěź(žěÖ‚ąôŪáīžõź žßĄŽč®Ž™Ö ÍĶ≠ž†úžßąŽ≥ĎŽ∂ĄŽ•ė-10 žĹĒŽďú: M303)Ž•ľ ŽĆÄžÉĀžúľŽ°ú žčúŪĖČŪĖąŽč§. ŪÉÄžõź žĚīžÜ°, Ž∂ąžôĄž†Ą ŽėźŽäĒ žě¨Žįú ÍįÄžôÄžā¨Ūā§Ž≥Ď, Žį©Ž¨ł ž†Ą IVIG Ūą¨žó¨, žóī žßÄžÜćÍłįÍįĄžĚī Ž∂ąŽ™ÖŪôēŪēú ŪôėžěźŽäĒ ž†úžôłŪĖąŽč§. Ž≥ł žóįÍĶ¨ŽäĒ Í≤ĹžÉĀŽĆÄŪēôÍĶźŽ≥Ďžõź žěĄžÉĀžóįÍĶ¨žč¨žĚėžúĄžõźŪöĆ žäĻžĚłžĚĄ žĖĽžĚÄ ŪõĄ žčúŪĖČŪĖąŽč§(IRB No. GNUH 2018-04-020).
žóįÍĶ¨ŽĆÄžÉĀžěźžĚė žĚėŽ¨īÍłįŽ°ĚžĚĄ ŪõĄŪĖ•ž†ĀžúľŽ°ú Ž∂ĄžĄĚŪĖąŽč§. žěĄžÉĀž†Ā ŪäĻžĄĪžúľŽ°ú Ūôėžěź ŽāėžĚī(žõĒ) ŽįŹ žĄĪŽ≥Ą, žóī žßÄžÜćÍłįÍįĄ, žĚĎÍłČžč§ Žį©Ž¨ł ŽįŹ žĶúžĘÖ žßĄŽč® žčú ÍįĀÍįĀ ŽßĆž°ĪŪēėŽäĒ ÍįÄžôÄžā¨Ūā§Ž≥Ď žßĄŽč®Íłįž§ÄžĚĄ žąėžßĎŪĖąŽč§. ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßąžĚĄ ŪŹ¨Ūē®Ūēú Ūėąžē°Í≤Äžā¨(Žį©Ž¨ł ŽčĻžčú žĪĄŪėą) Ūē≠Ž™©žúľŽ°ú ŽįĪŪėąÍĶ¨ žąė, ž†ąŽĆÄž§ĎžĄĪÍĶ¨ žąė, Ž∂ĄžóĹŪēĶž§ĎžĄĪÍĶ¨ ŽįŹ Ž¶ľŪĒĄÍĶ¨ Ž∂Ąžú®, ŪėąžÉČžÜĆ, ŪėąžÜĆŪĆź, C-ŽįėžĚώ讎įĪžßą, ž†ĀŪėąÍĶ¨žĻ®ÍįēžÜ掏Ą, žēĆŽ∂ÄŽĮľ, ŽāėŪ䳎•®, žēĄžä§ŪĆĆŽ•īŪÖĆžĚīŪäł ŽįŹ žēĆŽĚľŽčĆ žēĄŽĮłŽÖłž†ĄŽč¨Ūö®žÜĆ, NT-proBNPŽ•ľ žąėžßĎŪĖąŽč§. žėąŪõĄ Ž≥ÄžąėŽ°ú IVIG Ūą¨žó¨ žó¨Ž∂Ä ŽįŹ žčúž†ź(Žįúžóī Íłįž§Ä), IVIG Ž∂ąžĚĎžĄĪ žó¨Ž∂Ä, žĚĎͳȞč§(žčúÍįĄ) ŽįŹ Ž≥Ďžõź(žĚľ) ž≤īŽ•ėžčúÍįĄ, žč¨žīąžĚĆŪĆĆŽ°ú ŪôēžĚłŪēú ÍīÄžÉĀŽŹôŽß•Ūē©Ž≥Ďž¶Ě žú†Ž¨īŽ•ľ ž°įžā¨ŪĖąŽč§. IVIG Ž∂ąžĚĎžĄĪ žó¨Ž∂ÄŽäĒ IVIG ž≤ę Ūą¨žó¨ ŪõĄ 48žčúÍįĄ žĚīžÉĀ žóīžĚī žßÄžÜćŪēėŽäĒ Í≤ÉžúľŽ°ú ž†ēžĚėŪĖąŽč§[7].
ÍįÄžôÄžā¨Ūā§Ž≥ĎžĚÄ 2017ŽÖĄ ŽĮłÍĶ≠žč¨žě•ŪėĎŪöĆ(American Heart Association) žßĄŽč®Íłįž§ÄžĚĄ Í∑ľÍĪįŽ°ú, 5žĚľ žĚīžÉĀ žßÄžÜćŪēėŽäĒ žóīÍ≥ľ ž£ľžöĒ žěĄžÉĀž¶ĚžÉĀ 5Íįú ž§Ď 4Íįú žĚīžÉĀžĚĄ ŽßĆž°ĪŪēėŽäĒ ŪôėžěźŽ•ľ žôĄž†Ą ÍįÄžôÄžā¨Ūā§Ž≥ĎžúľŽ°ú žßĄŽč®ŪĖąŽč§[1]. žóī žßÄžÜćÍłįÍįĄ(Žįúžóī ŽčĻžĚľžĚĄ 1žĚľŽ°ú Í≥Ąžāį)žĚī 5žĚľ ŽĮłŽßĆ ŽįŹ 5žĚľ žĚīžÉĀžĚł ŪôėžěźŽ•ľ ž°įÍłį ŽįŹ ŪõĄÍłį Žį©Ž¨łÍĶįžúľŽ°ú ÍįĀÍįĀ ž†ēžĚėŪĖąŽč§.
žóįžÜćŪėē Ž≥ÄžąėŽäĒ ž†ēÍ∑úŽ∂ĄŪŹ¨ žó¨Ž∂Äžóź ŽĒįŽĚľ ŪŹČÍ∑† ŽįŹ ŪĎúž§ÄŪéłžį® ŽėźŽäĒ ž§ĎžēôÍįí ŽįŹ žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄŽ°ú ÍįĀÍįĀ Íłįžą†ŪĖąŽč§. Ž≤Ēž£ľŪėē Ž≥ÄžąėŽäĒ Ūôėžěź žąėžôÄ ŽįĪŽ∂Ąžú®Ž°ú Íłįžą†ŪĖąŽč§. ž°įÍłį ŽįŹ ŪõĄÍłį Žį©Ž¨łÍĶįžĚė ŽĻĄÍĶźŽäĒ žóįžÜćŪėē Ž≥ÄžąėŽäĒ Student t-testžôÄ Mann-Whitney U testŽ°ú, Ž≤Ēž£ľŪėē Ž≥ÄžąėŽäĒ chi-square testŽ°ú, ÍįĀÍįĀ Ž∂ĄžĄĚŪĖąŽč§. ŪÜĶÍ≥Ą ŪĒĄŽ°úÍ∑łŽě®žúľŽ°ú SPSS ver. 21.0 (IBM Co., Armonk, NY)žĚĄ žĚīžö©ŪĖąÍ≥†, P < 0.05Ž•ľ ŪÜĶÍ≥Ąž†ĀžúľŽ°ú žú†žĚėŪēėŽč§Í≥† ž†ēžĚėŪĖąŽč§.
Í≤į Í≥ľ
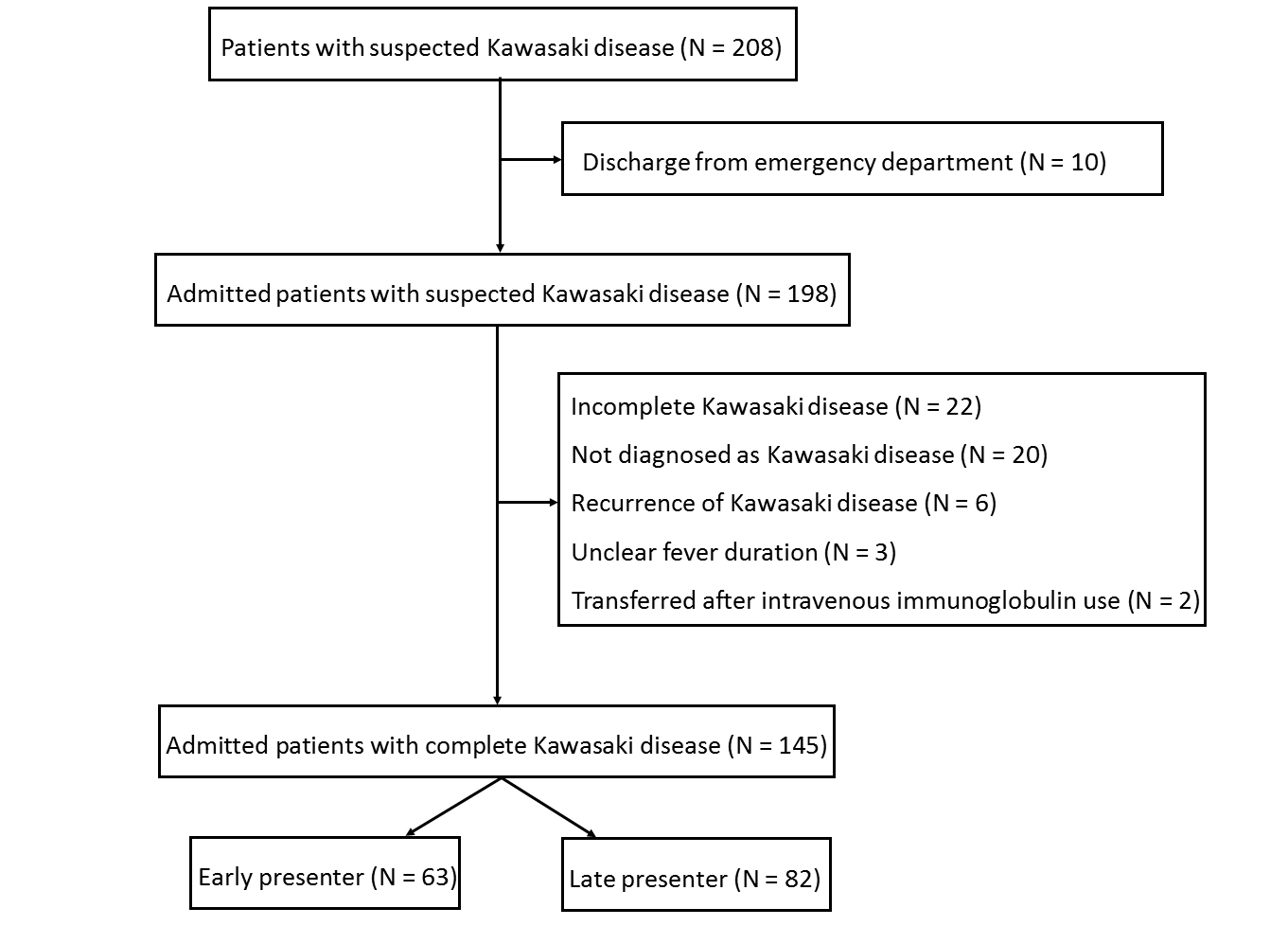
žóįÍĶ¨ÍłįÍįĄžóź Ž≥łžõź žĚĎͳȞ觞̥ Žį©Ž¨łŪēú ÍįÄžôÄžā¨Ūā§Ž≥Ď žĚėžč¨ Ūôėžěź 208Ž™Ö ž§Ď, 63Ž™ÖžĚĄ ž†úžôłŪēú žīĚ 145Ž™ÖžĚė žôĄž†Ą ÍįÄžôÄžā¨Ūā§Ž≥Ď ŪôėžěźŽ•ľ žóįÍĶ¨ŽĆÄžÉĀžěźŽ°ú ž†ēžĚėŪĖąŽč§(Fig. 1). ŽāėžĚī ž§ĎžēôÍįížĚÄ 27.0ÍįúžõĒ(žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 12.0-46.5ÍįúžõĒ)žĚīžóąÍ≥†, žĚī ž§Ď Žā®žěźÍįÄ 87Ž™Ö(60.0%)žĚīžóąŽč§. ŪŹČÍ∑† žóī žßÄžÜćÍłįÍįĄžĚÄ 4.7 ¬Ī 1.8žĚľ(ž§ĎžēôÍįí 5.0žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 4.0-6.0žĚľ])žĚīžóąŽč§. Ž™®Žď† ŪôėžěźžóźÍ≤Ć IVIGžôÄ žēĄžä§ŪĒľŽ¶įžĚĄ Ūą¨žó¨ŪĖąŽč§. ž°įÍłį Žį©Ž¨łÍĶį(63Ž™Ö[43.4%])žĚÄ ŪõĄÍłį Žį©Ž¨łÍĶįŽ≥īŽč§ žú†žĚėŪēėÍ≤Ć žĖīŽ¶į ŽāėžĚī(17.0ÍįúžõĒ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 7.0-45.0ÍįúžõĒ] vs. 32.5ÍįúžõĒ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 14.0-48.0ÍįúžõĒ]; P = 0.006), žßßžĚÄ žóī žßÄžÜćÍłįÍįĄ(3.0žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 2.0-4.0žĚľ] vs. 6.0žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 5.0-7.0žĚľ]; P < 0.001)Ž•ľ Ž≥īžėÄŽč§. žĚĎÍłČžč§ Žį©Ž¨ł ŽčĻžčú ŽßĆž°ĪŪēėŽäĒ žßĄŽč®Íłįž§Ä ÍįúžąėŽäĒ ž°įÍłį Žį©Ž¨łÍĶįžóźžĄú ŽćĒ ž†ĀžóąžßÄŽßĆ(1.0Íįú[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 0.0-4.0Íįú] vs. 4.0Íįú[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 3.0-4.0Íįú]; P < 0.001), žĶúžĘÖ žßĄŽč® žčúžóź ŽßĆž°ĪŪēėŽäĒ žßĄŽč®Íłįž§Ä ÍįúžąėŽäĒ ŽĎź ÍĶį ÍįĄ žį®žĚīŽ•ľ Ž≥īžĚīžßÄ žēäžēėŽč§(Table 1).
ž°įÍłį Žį©Ž¨łÍĶįžĚī ŪõĄÍłį Žį©Ž¨łÍĶįŽ≥īŽč§ ŽāģžĚÄ ŪėąžÜĆŪĆź žąėŽ•ľ Ž≥īžĚł Í≤É(336.7 ¬Ī 105.2 [103/mm3] vs. 381.6 ¬Ī 121.8 [103/mm3]; P = 0.02) žôłžóź ÍłįŪÉÄ ÍłČžĄĪÍłįŽįėžĚĎŽ¨ľžßą žąėžĻėŽäĒ ŽĎź ÍĶį ÍįĄ žį®žĚīÍįÄ žóÜžóąŽč§. NT-proBNPŽäĒ 33Ž™ÖžĚė ŪôėžěźžóźžĄú ŪôēžĚłŪĖąÍ≥†, ŽĎź ÍĶį ÍįĄ žį®žĚīÍįÄ žóÜžóąŽč§(Table 2).
IVIG Ūą¨žó¨ žčúž†źžĚÄ ž°įÍłį Žį©Ž¨łÍĶįžóźžĄú žú†žĚėŪēėÍ≤Ć žßßžēėžßÄŽßĆ(5.0žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 4.0-5.0žĚľ] vs. 6.0žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 5.0-7.0žĚľ]; P < 0.001), IVIG Ž∂ąžĚĎžĄĪ ŽįŹ ÍīÄžÉĀŽŹôŽß• Ūē©Ž≥Ďž¶Ě(Ž™®ŽĎź žĘĆžł°ž£ľÍīÄžÉĀŽŹôŽß•[left main coronary artery] Ūôēžě•)žĚÄ ŽĎź ÍĶį ÍįĄ žį®žĚīÍįÄ žóÜžóąŽč§. žĚĎÍłČžč§ ŽįŹ Ž≥Ďžõź ž≤īŽ•ėÍłįÍįĄžĚÄ ž°įÍłį Žį©Ž¨łÍĶįžóźžĄú ŽćĒ ÍłłžóąŽč§(3.9žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 2.4-5.7žĚľ] vs. 2.8žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 1.6-4.2žĚľ]; P = 0.001) (7.0žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 6.0-8.0žĚľ] vs. 6.0žĚľ[žā¨Ž∂ĄžúĄžąė Ž≤ĒžúĄ, 5.0-7.0žĚľ]; P = 0.003) (Table 2).
Í≥† žįį
Ž≥ł žóįÍĶ¨žóźžĄú Žįúžóī 5žĚľ žĚīž†Ąžóź Žį©Ž¨łŪēú ÍįÄžôÄžā¨Ūā§Ž≥Ď ŪôėžěźÍįÄ 5žĚľ žĚīŪõĄžóź Žį©Ž¨łŪēú ŪôėžěźŽ≥īŽč§ ŽćĒ ŽāģžĚÄ ŪėąžÜĆŪĆź žąėŽ•ľ Ž≥īžėÄžßÄŽßĆ, Žč§Ž•ł ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßą žąėžĻėžóźŽäĒ žį®žĚīÍįÄ žóÜžóąŽč§. Í∑łŽ¶¨Í≥† žĚī ŪôėžěźÍĶįžóźžĄú IVIGŽ•ľ ŽćĒ ž°įÍłįžóź Ūą¨žó¨ŪĖąžßÄŽßĆ, IVIG Ž∂ąžĚĎžĄĪ ŽįŹ ÍīÄžÉĀŽŹôŽß• Ūē©Ž≥Ďž¶Ě ŽĻąŽŹĄžóź žį®žĚīÍįÄ žóÜžóąÍ≥† ž≤īŽ•ėÍłįÍįĄžĚÄ žė§Ū칎†§ ŽćĒ ÍłłžóąŽč§.
ÍįÄžôÄžā¨Ūā§Ž≥ĎžĚė Í≤ĹÍ≥ľŽäĒ ͳȞĄĪÍłį, žēĄÍłČžĄĪÍłį, ŪöĆŽ≥ĶÍłįŽ°ú ŽāėŽČúŽč§[14]. ͳȞĄĪÍłįžóź žóīžĚĄ ŪŹ¨Ūē®Ūēú žěĄžÉĀž¶ĚžÉĀžĚī ŽįúžÉĚŪēėÍ≥†, žēĄÍłČžĄĪÍłįžóź žóīÍ≥ľ žěĄžÉĀž¶ĚžÉĀžĚī žā¨ŽĚľžßÄÍłį žčúžěĎŪēėŽ©į, ŪöĆŽ≥ĶÍłįŽ°ú žĚīžĖīžßĄŽč§. ͳȞĄĪÍłįžóź ŽįĪŪėąÍĶ¨ žąė, C-ŽįėžĚώ讎įĪžßą ŽÜ掏Ą, ž†ĀŪėąÍĶ¨žĻ®ÍįēžÜ掏ĄÍįÄ ÍįÄžě• ŽÜíÍ≥†(ŽßéÍ≥†), žēĄÍłČžĄĪÍłįžóź ŪėąžÜĆŪĆź žąėÍįÄ ÍįÄžě• ŽßéžúľŽ©į, ŪöĆŽ≥ĶÍłįžóź Ž¶ľŪĒĄÍĶ¨ žąėÍįÄ ÍįÄžě• ŽßéŽč§Í≥† žēĆŽ†§ž°ĆŽč§[12]. Ž≥ł žóįÍĶ¨žóźžĄú ͳȞĄĪÍłįžóź ž¶ĚÍįÄŪēėŽäĒ ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßąžĚÄ ŽĎź ÍĶį ÍįĄ žį®žĚīÍįÄ žóÜžóąžßÄŽßĆ, ŪėąžÜĆŪĆź žąė(žēĄÍłČžĄĪÍłįžóź ž¶ĚÍįÄ)ŽäĒ ž°įÍłį Žį©Ž¨łÍĶįžóźžĄú žú†žĚėŪēėÍ≤Ć ž†ĀžóąŽč§. žĚīŽäĒ ŪėąžÜĆŪĆźž¶ĚÍįÄž¶ĚžĚī ŽöúŽ†∑ŪēėžßÄ žēäžĚÄ ÍłČžĄĪÍłįžóźŽŹĄ[1], žóī žßÄžÜćÍłįÍįĄžóź ŽĒįŽĚľ ŪėąžÜĆŪĆź žąėžóź žį®žĚīÍįÄ žěąžĚƞ̥ žčúžā¨ŪēúŽč§.
Ž≥ł žóįÍĶ¨žóźžĄú ž°įÍłįŽį©Ž¨łÍĶį ŪôėžěźžĚė ŽāėžĚīÍįÄ žĖīŽ¶¨Í≥†, ŽßĆž°ĪŪēėŽäĒ žßĄŽč®Íłįž§Ä ÍįúžąėÍįÄ ž†ĀžúľŽ©į, žĚĎÍłČžč§ ž≤īŽ•ėÍłįÍįĄžĚī ŽćĒ ÍłłžóąŽč§. žĚīŽäĒ žßĄŽč®žĚė žĖīŽ†§žõÄžúľŽ°ú žĚłŪēú ž≤īŽ•ėÍłįÍįĄ ž¶ĚÍįÄŽ•ľ žčúžā¨ŪēúŽč§. ÍįÄžôÄžā¨Ūā§Ž≥Ď žßĄŽč®Íłįž§ÄžĚĄ ŽßĆž°ĪŪēėžßÄ žēäŽäĒ ŪôėžěźžóźžĄú Žč§Ž•ł žóī ÍīÄŽ†® žßąŪôėÍ≥ľžĚė ÍįźŽ≥ĄžĚĄ žúĄŪēī ŽįĪŪėąÍĶ¨ žąė, ŪėąžÜĆŪĆź žąė, C-ŽįėžĚώ讎įĪžßą, ž†ĀŪėąÍĶ¨žĻ®ÍįēžÜ掏Ą ŽďĪžĚī žú†žö©ŪēėŽč§[5,8,15]. Ž≥ł žóįÍĶ¨žóźžĄú žĪĄŪėą žčúÍłį(ž¶Č 5žĚľ žĚīž†ĄÍ≥ľ žĚīŪõĄ)žóź ŽĒįŽ•ł ŽįĪŪėąÍĶ¨ žąė, C-ŽįėžĚώ讎įĪžßą, ž†ĀŪėąÍĶ¨žĻ®ÍįēžÜ掏ĄžĚė ŽĎź ÍĶį ÍįĄ žį®žĚīÍįÄ žóÜžóąžúľŽĮÄŽ°ú, žĚī ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßą Í≤Äžā¨Ž•ľ ÍįźŽ≥ĄžßĄŽč®žóź Ūôúžö©Ūē† žąė žěąžĚĄ Í≤ÉžĚīŽč§.
ŽįėŽ©ī, Žįúžóī 5žĚľ žĚīž†Ąžóź Žį©Ž¨łŪēú ŪôėžěźžĚė ÍįźŽ≥ĄžßĄŽč®žóź ŪėąžÜĆŪĆź žąėŽ•ľ Ūôúžö©ŪēėÍłįžóźŽäĒ ž†úŪēúž†źžĚī žěąžĚĄ Í≤ÉžúľŽ°ú ž∂Ēž†ēŪēúŽč§. ŪŹźŽ†ī, žÉĀÍłįŽŹĄÍįźžóľ ŽďĪÍ≥ľ ŽĻĄÍĶźŪēėžó¨ ÍįÄžôÄžā¨Ūā§Ž≥Ϟ󟞥ú ŪėąžÜĆŪĆź žąėŽäĒ žú†žĚėŪēėÍ≤Ć ŽÜížßÄŽßĆ, ž†ēžÉĀ Ž≤ĒžúĄ Žāī(žėą: < 336.7 ¬Ī 105.2 [103/mm3])žóź Ž∂ĄŪŹ¨ŪēúŽč§[5,8]. žĚīŽäĒ Ž≥ł žóįÍĶ¨žóźžĄú ŽĎź ÍĶįžĚė ŪėąžÜĆŪĆź žąėŽäĒ žú†žĚėŪēú žį®žĚīŽ•ľ Ž≥īžėÄžßÄŽßĆ, Ž™®ŽĎź ž†ēžÉĀ Ž≤ĒžúĄžóź Ž∂ĄŪŹ¨ŪĖąŽč§ŽäĒ ž†źÍ≥ľ žĚľŽß•žÉĀŪÜĶŪēúŽč§. ŽĒįŽĚľžĄú ŪėąžÜĆŪĆź žąėžóź Í∑ľÍĪįŪēú ÍįźŽ≥ĄžßĄŽč®žóź ž£ľžĚėÍįÄ ŪēĄžöĒŪēėŽč§. žč§ž†ú 2017ŽÖĄ žßĄŽč®Íłįž§ÄžóźžĄú ž†úžčúŪēú Ž∂ąžôĄž†Ą ÍįÄžôÄžā¨Ūā§Ž≥Ď žēĆÍ≥†Ž¶¨Žď¨žóź ŽĒįŽ•īŽ©ī, Žįúžóī 7žĚľ žĚīŪõĄžóź žčúŪĖČŪēú ŪėąžÜĆŪĆź žąėŽ•ľ Ūôúžö©Ūēīžēľ ŪēúŽč§[1]. žßĄŽč® žėĀžó≠ žôłžóź IVIGžóź ŽĆÄŪēú ž†ÄŪē≠žĚīŽāė Ūē©Ž≥Ďž¶Ě ŽįúžÉĚ žėąžł°žóźŽŹĄ Ūėąžē°Í≤Äžā¨ŽäĒ ŽßéžĚī žĚīžö©ŽźėÍ≥† žěąŽč§[16-20]. ŪĖ•ŪõĄ žĚī ž£ľž†úžóź ŽĆÄŪēú ž∂ĒÍįÄ žóįÍĶ¨ÍįÄ ŪēĄžöĒŪēėŽč§.
ž°įÍłį Žį©Ž¨łÍĶįžóźžĄú IVIG Ūą¨žó¨ žčúž†źžĚī ŽĻ®ŽěźžßÄŽßĆ, IVIG Ž∂ąžĚĎžĄĪ ŽįŹ ÍīÄžÉĀŽŹôŽß• Ūē©Ž≥Ďž¶Ě ŽĻąŽŹĄžóź žį®žĚīÍįÄ žóÜžóąÍ≥†, žė§Ū칎†§ ž≤īŽ•ėÍłįÍįĄžĚÄ ŽćĒ ÍłłžóąŽč§. ŽĒįŽĚľžĄú, IVIG Ūą¨žó¨ žčúž†źžóź ŽĆÄŪēú žßÄžĻ®žĚĄ žąėŽ¶ĹŪēėŽäĒ Žćįžóź žĚī ž†źžĚĄ Í≥†Ž†§Ūēīžēľ ŪēúŽč§.
Ž≥ł žóįÍĶ¨žĚė ž†úŪēúž†źžĚÄ Žč§žĚĆÍ≥ľ ÍįôŽč§. Žč®žĚľ ÍłįÍīÄ žóįÍĶ¨žóź Žāīžě¨Ūēú žßÄžó≠ž†Ā ŪäĻžĄĪÍ≥ľ ž†úŪēúŽźú Ūôėžěź žąėŽ°ú Ž≥ł žóįÍĶ¨ Í≤įÍ≥ľŽ•ľ žĚľŽįėŪôĒŪēėŽäĒ Í≥ľž†ēžóź žĖīŽ†§žõÄžĚī žěąžĚĄ žąė žěąŽč§. Í∑łŽ¶¨Í≥† žĚľŽ∂Ä žĚėŽ¨īÍłįŽ°Ě žė§Ž•ėÍįÄ žóįÍĶ¨ Í≤įÍ≥ľžóź ŽĻĄŽö§Ž¶ľžĚĄ žīąŽěėŪĖąžĚĄ žąė žěąŽč§. NT-proBNPŽ•ľ žčúŪĖČŪēú Ūôėžěź žąėÍįÄ ž†ĀžĖī, žĚīŽ•ľ Ūö®Í≥ľž†ĀžúľŽ°ú Ž∂ĄžĄĚŪēėžßÄ Ž™ĽŪĖąŽč§.
Í≤įŽ°†ž†ĀžúľŽ°ú, Žįúžóī 5žĚľ žĚīž†Ąžóź Žį©Ž¨łŪēú ÍįÄžôÄžā¨Ūā§Ž≥Ď ŪôėžěźŽäĒ 5žĚľ žĚīŪõĄžóź Žį©Ž¨łŪēú ŪôėžěźŽ≥īŽč§ ŪėąžÜĆŪĆź žąėŽäĒ žú†žĚėŪēėÍ≤Ć ŽāģžēėÍ≥†, ŽįĪŪėąÍĶ¨ žąė, C-ŽįėžĚώ讎įĪžßąžóźŽäĒ žį®žĚīÍįÄ žóÜžóąŽč§. Í∑łŽ¶¨Í≥† ž†ĄžěźžĚė ŪôėžěźÍĶįžóź IVIGŽ•ľ ž°įÍłįžóź Ūą¨žó¨ŪĖąžßÄŽßĆ, žėąŪõĄžĚė žį®žĚīŽäĒ žóÜžóąŽč§. ÍįÄžôÄžā¨Ūā§Ž≥Ď ŪôėžěźžóźžĄú žóī žßÄžÜćÍłįÍįĄžóź ŽĒįŽ•ł ͳȞĄĪÍłįŽįėžĚĎŽ¨ľžßą žąėžĻėžĚė žį®žĚīŽ•ľ žĚīŪēīŪēėÍ≥†, žĚīŽ•ľ ÍįźŽ≥ĄžßĄŽč®žóź Ūôúžö©ŪēėŽäĒ Í≤ÉžĚī ŪēĄžöĒŪēėŽč§.