Introduction
Simple facial laceration (henceforth facial laceration, unless otherwise specified) is a common complaint in pediatric emergency departments (PEDs). Facial lacerations cause much concern for outcomes by guardians of children with the lacerations. Following wound cleansing, most children require wound repairs, such as suture (1-4). Relevant literature provides sparse information on cosmetic outcomes of facial lacerations sutured by plastic surgery (PS) residents or pediatric emergency physicians (PEPs) (5-8). Such outcomes need to be rated using various tools, such as the Stony Brook scar (SBS) score, which has been validated (9).
In Israel, most sutures for facial lacerations in PEDs are performed by PEPs or PS residents. PEPs have completed residency in pediatrics and fellowship in pediatric emergency medicine. PS residents are in a postgraduate year 1-5. Although most sutures had been performed by PS residents, PEPs have been performing the procedures in recent years when there are more trained PEPs in Israel. Simple lacerations, not limited to the face, account for approximately 4% of PED visits in Israel (10).
In this study, children who underwent facial laceration sutures in a PED in Israel were assessed for their cosmetic outcomes, such as scar, within approximately 1 year of the sutures. The hypothesis was that the outcomes were comparable between PEPs and PS residents.
Methods
This study was a single-center, retrospective study using a convenience sample. The study population included children who were sutured in the PED of Shaare Zedek Medical Center, Jerusalem, Israel from 2020 through 2022 with at least 1-year follow-up from the suturing. The study was approved by the hospital’s Helsinki committee institutional review board (IRB no. SZMC-20-0552).
Children with discharge diagnosis of facial laceration were eligible to participate. Informed consents were obtained from their legal guardians who were randomly extracted from the hospital’s electronic databases. Those with incomplete records or missing contact information were excluded. To minimize positive-intention selection bias, the study purpose of comparing the performers of sutures was not revealed during the participant selection process. To calculate statistical power, minimum of 50 children were included respectively for the children sutured by PEPs (PEP group) and by PS residents (PS group).
Once informed consents were obtained, the guardians were asked to provide high-quality digital photographs of the wounds from 5 different angles, including close-up and distant images. In addition, the guardians were asked to rate the cosmetic outcomes using a general numeric score (GNS) ranging from 0 to 100. The photographs received were presented to 3 doctors blinded to who performed the sutures: 2 plastic surgeons (an attending and a resident) and 1 PEP (attending). The 3 doctors rated the outcomes using the SBS score (11) as well as the GNS.
To compare categorical and continuous variables, we used the chi-square or Fisher exact tests and 2-sample t-tests, respectively. Assessing the differences between the scores rated by 2 different raters was done by McNemar tests. The Kappa measurement of interrater reliability, as well as the weighted Kappa (using linear weights), was used for estimating the degree of agreement between 2 raters. The association among 3 raters was assessed by calculating the intraclass correlation coefficient (ICC). All tests applied were 2-tailed, and a P value of 0.05 or less was considered significant. Statistical analyses were performed by a statistician in the Faculty of Medicine using IBM SPSS Statistics for Windows, version 22 (IBM Corp.)
Results
We obtained informed consents from the guardians of 108 (82.4%) among a total of 131 children sutured in the PED. Their follow-up period ranged from 12 to 14 months. Of the 108 children whose median age was 4.0 years (interquartile range, 3.0-7.0), 57 and 51 were sutured by PEPs and PS residents, respectively. The PEPs had a minimum of 1-year post-fellowship experience, whereas the PS residents had a 3.2 mean postgraduate year (standard deviation, 1.2).
Baseline characteristics are compared in Table 1. Facial lacerations were located mostly on the forehead (48.1%), lips (13.9%), eyebrow (12.0%) and chin (11.1%). Only 38 children had records regarding the lengths of wounds. None of the records detailed depths. The mean lengths were comparable between the 2 groups (PEP [25 children], 1.9 ± 0.8 cm vs. PS [13 children], 2.1 ± 0.4 cm; P = 0.176). Non-absorbable sutures were used in 91 children (84.3%), with the rest using absorbable or combined suturing. No records were found in the discharge letters regarding complicated lacerations. Of the 42 children (38.9%) undergoing procedural sedation, 38, 1, and 3 were given intranasal midazolam, nitrous oxide, and ketamine, respectively, without any adverse events. The sedation was more frequently used in the PS group (Table 1).
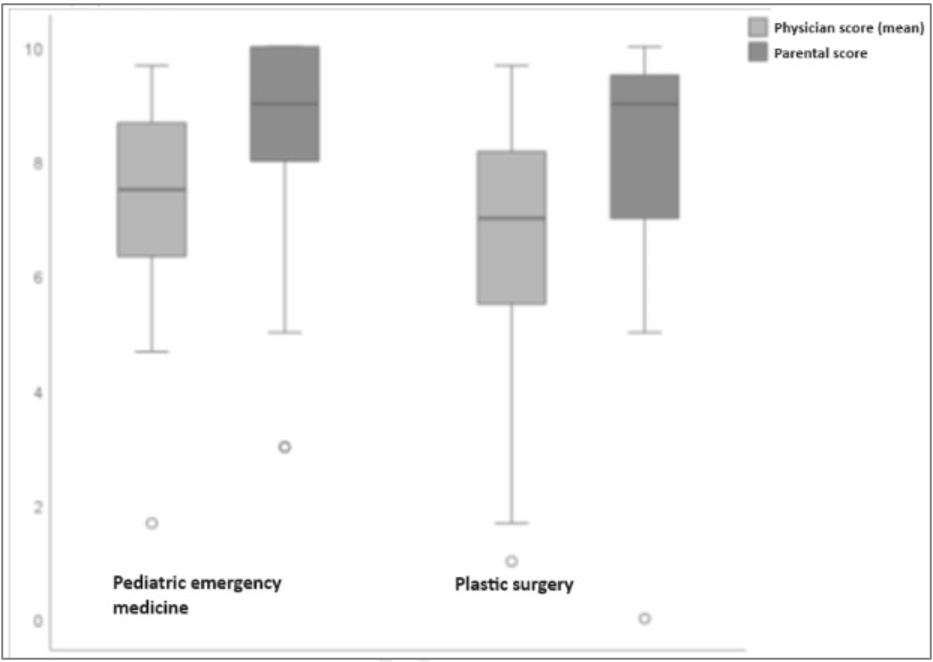
Guardian-rated median GNS showed no difference between the 2 groups (PEP, 90.0 [interquartile range, 70.0-95.0] vs. PS, 90.0 [60.0-90.0]; P = 0.310) (Fig. 1). In contrast, doctor-rated median GNS was higher in the PEP group (PEP, 75.0 [63.3-86.7] vs. PS, 70.0 [53.3-83.3]; P = 0.046). The overall median SBS score for the study population was 3.4 (2.9-3.8) with comparable median scores of the 2 groups (PEP, 4.0 [3.0-4.0] vs. PS, 4.0 [2.5-4.0]; P = 0.205) (Fig. 2). An SBS score of 3 or higher was similarly frequent in both groups (PEP, 87.7% vs. PS, 74.5%; P = 0.173). The Kappa score was low (0.36; 95% confidence interval, 0.23-0.54) with a Cronbach’s alpha of 0.77. However, the ICC was substantial (0.77; 0.68-0.84).
Discussion
This study shows overall favorable long-term cosmetic outcomes of facial lacerations rated by guardians as well as by doctors, suggesting that with appropriate training, most facial lacerations could heal well following sutures. In addition, the doctor-rated median GNS was higher in the children sutured by the PEPs, compared with the equivalent value of those sutured by the PS residents. This finding indicates that PEPs may be as competent as PS residents in suturing the lacerations. The interrater reliability was low between the assessing doctors whereas the ICC was substantial. Despite the overall favorable cosmetic outcomes, the degree of acceptable outcomes may vary depending on each doctor’s specialty, expertise, or clinical experience.
Regarding GNS, the guardian-rated median values were higher than the doctor-rated median values (Fig. 1). This may show that the guardians did not expect the level of perfection as perceived by the doctors. This has been shown in a previous study using digital images (11). It may be worth mentioning, given the median age of the study population (4 years), the small percentage used procedural sedation for facial lacerations. A PEP who is well-versed in working with the pediatric population may use non-pharmacologic techniques to circumvent the potential adverse effects of sedatives or anxiolytics.
This study has some limitations. First, the single-center, retrospective study design and setting limit its interpretation. In addition, several confounders exist. Second, convenience sampling might lead to a potentially higher rate of participation from the guardians satisfied with the cosmetic outcomes. However, no guardians refused participation based on dissatisfaction. Third, inherently, the use of 2-dimensional photographs might limit the reliability of wound assessment, compared with a live assessment. This potential flaw could be exaggerated by that the raters had not been trained in assessing the outcomes using photographs. We tried to minimize such possibilities by using images from different angles. Despite the limitations, this study confers an overall appreciation of the cosmetic outcomes according to PEPs or PS residents.
In conclusion, this study shows that long-term cosmetic outcomes of facial lacerations are overall favorable without differences between PEPs and PS residents performing sutures. This strengthens the knowledge on the quality of suturing performed by PEP and PS residents in the emergency department setting.