Introduction
The tongue can be entrapped in a bottle when a vacuum is created inside. If the entrapment prolongs, painful lingual edema may lead to agitation, necrosis, or upper airway obstruction (UAO). These sequelae can be prevented by early reduction. The unique situation may need a reduction or removal procedure under general anesthesia (1-3). To bypass the potential risk of anesthesia, the entrapped tongue needs to be reduced non-invasively by applying positive pressure (PP) as an initial measure in emergency departments (EDs) (4,5).
Case
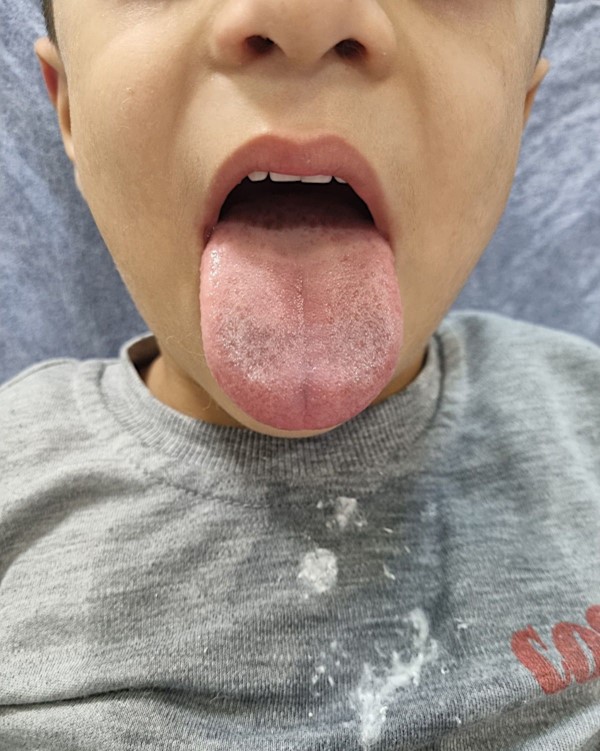
A previously healthy, 5-year-old boy tried to drink water from a glass bottle before going to sleep, and his tongue became entrapped in the bottle due to the vacuum effect. His parents failed to extract the tongue from the bottle using olive oil. Forty-five minutes after the event, the boy was brought to the ED, and evaluated by an emergency physician (EP). The initial vital signs were as follows: blood pressure, 100/65 mmHg; heart rate, 125 beats/minute; respiratory rate, 23 breaths/minute; temperature, 36.9 °C; and oxygen saturation, 99% on room air. Notably, the distal part of the tongue entrapped in the bottle was highly edematous and ecchymotic (Fig. 1). At that time, he was agitated and drooling without dyspnea.
The EP tried to reduce the tongue from the bottle using lubricant gel and traction, but failed. After a subsequent consultation with a pediatric and an orthopedic surgeon, they decided to reduce the tongue by applying PP (2,3). Following the recommendations of the 2 surgeons, the EP successfully performed the procedure in the ED. A plastic 16-gauge intravenous cannula was inserted into the bottle from the side of the tongue, and 40 mL of air was injected into the bottle using a syringe via the cannula. Consequently, the tongue was easily reduced without any damage. Given the stable vital signs and short procedure time, procedural sedation and analgesia (PSA) was not applied to the boy. After a 2-hour observation in the ED, the lingual edema and ecchymosis were resolved, and he became able to eat (Fig. 2). Finally, he was discharged uneventfully. At the 2-week follow-up, the boy complained about nothing with the tongue fully recovered.
Discussion
It is rare to encounter a child with the tongue entrapped in an object in EDs. In the literature, most patients were aged 11 years or younger, with the exception of a 28-year-old man with autism (5,6). While children are drinking from a glass bottle, plastic bottle, or aluminum can, they may try to absorb last drops of liquid from the bottle or can, or play with it. This behavioral tendency was reproduced in our case, where the boy created a vacuum in the bottle, leading to the tongue entrapment (1,5). The entrapment can lead to risky conditions, such as edema, UAO, and necrosis despite its wide collateral network.
Tongue entrapment can be relieved by applying PP as in our case, breaking, or cutting the bottle with an instrument, such as a dental drill. In previous cases where PP was applied, PSA was implemented (6). If the entrapment continues, pain may be an important complaint, raising the children’s agitation. Such situations can be prevented by early visits to EDs and timely intervention. We considered the use of PSA unnecessary and potentially harmful given the procedure time and the risk of UAO or aspiration (7).
If advanced, the entrapped tongue develops UAO, making oxygen delivery via masks or endotracheal tubes difficult. In such cases, EPs may need to perform nasotracheal intubation, cricothyroidotomy, or tracheostomy (5,8).
Directly pulling the bottle, or using lubricant gel or oil may be ineffective in relieving the entrapped tongue, and even injure the tongue (7). It has been reported that the tongue was not released even after many holes were made to remove the remaining liquid in a metal bottle, and to eliminate the negative pressure during transport to an ED (9).
Although the ED belongs to a small state hospital where lacks critical care resources, it was possible to non-invasively reduce the entrapped tongue without sequelae in the early period. The early reduction obviated intubation, anesthesia, or a referral to an advanced medical facility.