Introduction
Gastric volvulus is a rare disease caused primarily by laxity of the gastric ligaments, or secondarily by para-esophageal hernia or other diaphragmatic hernia [1,2]. This entity is classified according to the axis of rotation. Organo-axial type is the volvulus that occurs when the stomach rotates along its long axis. The great curvature passes anteriorly but is displaced posteriorly. In the less common mesentero-axial volvulus, the stomach rotates along the short axis, resulting in the antrum and pylorus lying antero-superior to the gastroesophageal junction [1-5]. Acute gastric volvulus is a surgical emergency. A case of acute primary gastric volvulus in a 12-year-old girl is reported here with literature review, approved by the institutional review board of Dong-A University College of Medicine (IRB no. DAUHIRB-21-220).
Case
A previously healthy, 12-year-old girl visited the emergency department for abdominal pain lasting for 2 hours. Initial vital signs were as follows: blood pressure, 110/60 mmHg; heart rate, 78 beats per minute; respiratory rate, 20 breaths per minute; temperature, 36.3‚ĄÉ, and oxyhemoglobin saturation, 98%. Initial physical examination showed a good appearance, and the soft and non-tender abdomen.
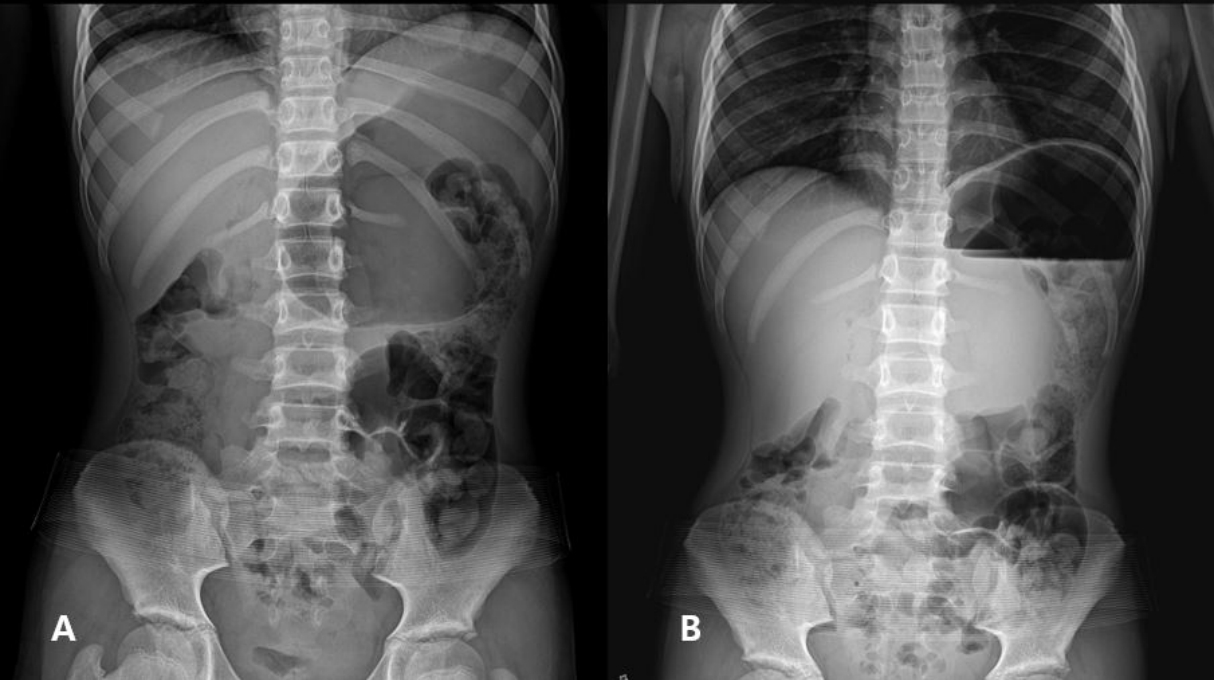
Laboratory findings, such as hemoglobin, C-reactive protein, amylase, lipase, and transaminases, were within the normal ranges. Plain radiographs showed gastric distension with air-fluid level (Fig. 1). During the emergency department stay, her abdominal pain was aggravated. Computed tomography (CT) showed severe gastric distension without ischemia, mass lesion or inflammatory focus with the unclear duodenojejunal junction (Fig. 2).
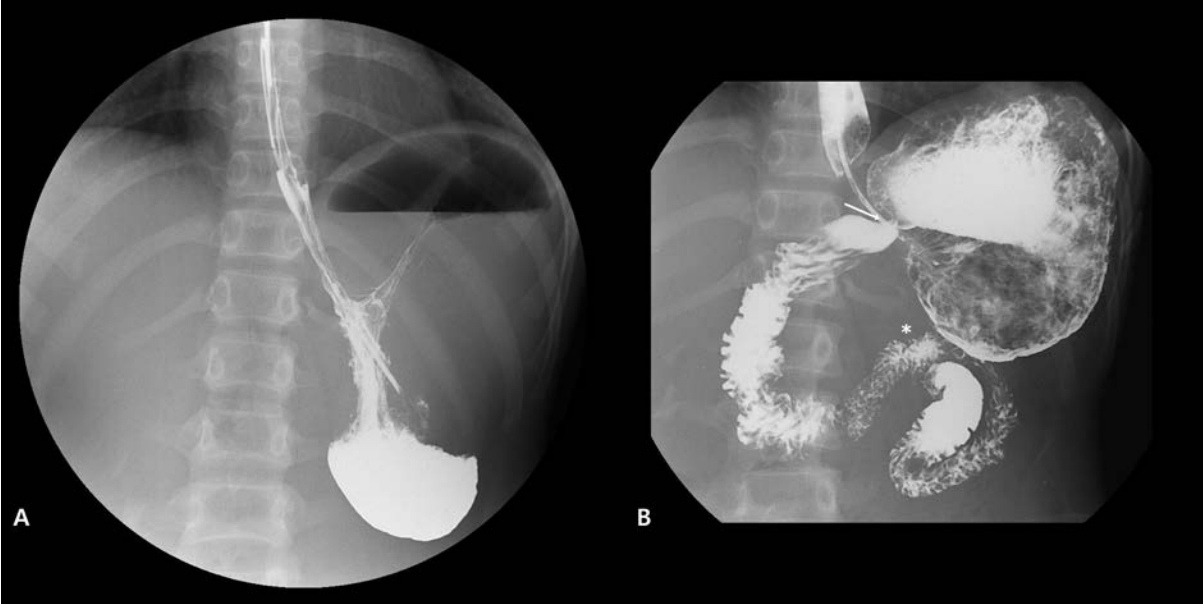
Subsequently, a pediatrician obtained surgical consultation for acute gastric distension with unknown causes. To relieve epigastric area tenderness with swelling noticed on a follow-up examination, a nasogastric tube was inserted to decompress the stomach. The gastric fluid decompressed through the tube was approximately 4,000 mL in volume and non-bilious in color. Given the unclear duodenojejunal junction on CT, upper gastrointestinal series (UGI) was performed to check the presence of partial intestinal malrotation. The UGI depicted a delayed gastric emptying with organo-axial volvulus (Fig. 3).
On emergency laparotomy, the stomach was severely dilated and edematous, but looked pinkish without a gangrenous change. The greater curvature folded upward and forward with the fundus rotated posteroinferiorly. The author carefully reduced the volvulus, and confirmed the absence of a secondary cause. For gastropexy, the anterior wall of gastric body was sutured to the peritoneum with multiple non-absorbable sutures to make a natural gastric location and to prevent a recurrence. The girl could take sips of water after 1 day of the surgery, and recovered uneventfully. During the 6-month follow-up, she had not reported discomfort and recurrence.
Discussion
Gastric volvulus is an uncommon cause of non-bilious vomiting resulting from the rotation of the stomach. Darani et al. [3] reported 21 children aged 6 days-4.3 years who underwent surgery for the volvulus from 1992 through 2003. A systematic review showed 125 children with the volvulus that occurred at a median age of 24 months and vomiting as the most common presenting symptomn [4]. While 65.6% of the volvulus occurred during the first 12 months of life, 8.1% was diagnosed at the age of 6-12 years [5]. In Korea, several cases were reported [6-12]. Although the most common symptoms are non-bilious vomiting, and abdominal distention and pain [5], this triad is also found in many other gastrointestinal diseases. Given the rarity and affected age range, it is difficult to consider the volvulus a differential diagnosis in adolescents with gastric dilatation and abdominal pain [13]. In addition, overeating itself can radiographically show a gastric dilatation. A clue in the study patient was the unclear duodenojejunal junction on CT and the late-developing epigastric tenderness. In this case, the UGI finding prompted the correct diagnosis while excluding partial intestinal malrotation.
UGI and CT are helpful in diagnosing gastric volvulus [14]. Chiefly, UGI can show a type of volvulus by passage of radiocontrast. Mesentero-axial type usually has a secondary cause whereas organo-axial type is more commonly primary [15]. An asymptomatic diaphragmatic anomaly can be often presented with acute gastric volvulus [15], highlighting the need to pursue a secondary cause.
In many reports, gastric necrosis and/or perforation had occurred before surgery. Mortality of acute volvulus was 2.5-fold higher than that of chronic volvulus (6.7% vs. 2.7%) [5]. Timely surgery consists of detorsion of volvulus and gastropexy, leading to a favorable outcome. In a case of the necrosis or perforation, additional surgical procedures are needed. Secondary causes should be ruled out to prevent recurrences. The gastropexy, which the author performed, prevents an internal hernia through the space between the sutures [16].
This case suggests that epigastric pain with gastric distension may be caused by gastric volvulus. Suspicion of this surgical disease can be proven via UGI.