ņä£ļĪĀ
ņĢīļĀłļź┤ĻĖ░ļŖö ņÖĖļČĆ ļ¼╝ņ¦łņŚÉ ļīĆĒĢ£ ļ®┤ņŚŁļ░śņØæņØä ņØ╝ņ╗½ļŖöļŹ░, ņØ┤ļ¤¼ĒĢ£ ņĢīļĀłļź┤ĻĖ░ ņżæņŚÉņä£ ņĢäļéśĒĢäļØĮņŗ£ņŖżļŖö ņżæņ”Ø ņĢīļĀłļź┤ĻĖ░ ļ░śņØæņØ┤ Ēö╝ļČĆ, ĒśĖĒØĪĻ│ä ņ£äņןĻ┤ĆĻ│ä, ņŗ¼ĒśłĻ┤ĆĻ│äņŚÉ ļÅÖņŗ£ļŗżļ░£ņĀüņØĖ ĻĖēņä▒ ņ”ØņāüņØä ņØ╝ņ£╝ĒéżļŖö ņ¦łĒÖśņ£╝ļĪ£, ņ╣śļŻīĒĢśņ¦Ć ļ¬╗ĒĢśļ®┤ ņé¼ļ¦ØņŚÉ ņØ┤ļź╝ ņłś ņ׳ļŗż[1,2]. ņäĖĻ│äņĀüņ£╝ļĪ£ ņĢäļéśĒĢäļØĮņŗ£ņŖż ļ░£ņāØļźĀņØĆ ļ¬ģĒÖĢĒĢśĻ▓ī ņĢīļĀżņ¦Ćņ¦Ć ņĢŖņĢśļŖöļŹ░, ņØ┤ļŖö Ļ│╝Ļ▒░ņŚÉ ņ¦äļŗ© ĻĖ░ņżĆņØ┤ ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖņĢśĻ│Ā ņØśļŻīņ¦äņØ┤ ņĢäļéśĒĢäļØĮņŗ£ņŖżļź╝ ņĀ£ļīĆļĪ£ ņØĖņ¦ĆĒĢśņ¦Ć ļ¬╗ĒĢśņŚ¼ ņŗżņĀ£ļ│┤ļŗż ņĀüĻ▓ī ņ¦äļŗ©ņØä Ē¢łĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. Ļ│╝Ļ▒░ ņØīņŗØ ļśÉļŖö ņĢĮ ņĢīļĀłļź┤ĻĖ░ņØś ņØ╝ņóģņ£╝ļĪ£ ņāØĻ░üĒ¢łļŗżĻ░Ć, 2006ļģäĻ│╝ 2011ļģäņŚÉ ņāłļĪŁĻ▓ī ņĢäļéśĒĢäļØĮņŗ£ņŖż ņ¦äļŗ© ĻĖ░ņżĆ ļ░Å ņ¦äļŻīņ¦Ćņ╣©[1,3]ņØ┤ ļ░£Ēæ£ļÉśļ®┤ņä£ ņ¦äļŗ©ņØ┤ ņĀÉņĀÉ ļŖśņ¢┤ļéśļŖö ņČöņäĖņØ┤ļŗż. ĒĢśņ¦Ćļ¦ī ļ╣äĒŖ╣ņØ┤ņĀü ņ”ØņāüņØä ļ│┤ņØ┤Ļ▒░ļéś ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØ┤ ņŚåņ£╝ļ®┤ ņ×äņāü ņ¦äļŗ©ņØä ļåōņ╣Ā ņłś ņ׳ņ¢┤[4], ņØ┤ņŚÉ ļö░ļØ╝ ņŚÉĒö╝ļäżĒöäļ”░ Ēł¼ņŚ¼Ļ░Ć ļŖ”ņ¢┤ņĀĖ ņśłĒøäĻ░Ć ļéśļ╣Āņ¦ł ņłś ņ׳ļŗż[5,6]. ĒŖ╣Ē׳ 1-5ņäĖ ĒÖśņ×ÉļŖö ļŗżļźĖ ļéśņØ┤ļīĆļ│┤ļŗż ņĢäļéśĒĢäļØĮņŗ£ņŖżĻ░Ć ĒØöĒĢśĻ│Ā ļ│┤ņ▒ö, ņØīņŗØ Ļ▒░ļČĆ, ĻĄ¼ĒåĀ ļō▒ ļ╣äĒŖ╣ņØ┤ņĀü ņ”ØņāüņØ┤ ĒØöĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ņ×äņāü ņ¢æņāüņØś ļéśņØ┤ļīĆļ│ä ĒŖ╣ņ¦ĢņØ┤ ņ¦äļŗ©Ļ│╝ ņ╣śļŻīņŚÉ ņżæņÜöĒĢśļŗż[7]. ĒĢśņ¦Ćļ¦ī ĒĢ£ĻĄŁņŚÉņäĀ ņåīņĢä ņĢäļéśĒĢäļØĮņŗ£ņŖż ĒÖśņ×É ņŚ░ĻĄ¼Ļ░Ć ļČĆņĪ▒ĒĢ£ ņŗżņĀĢņØ┤ļŗż[8-10].
ļ│Ė ņĀĆņ×ÉļŖö ļŗ©ņØ╝ ņØæĻĖēņØśļŻīņä╝Ēä░ņŚÉ ļ░®ļ¼ĖĒĢ£ 18ņäĖ ņØ┤ĒĢś ņĢäļéśĒĢäļØĮņŗ£ņŖż ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņ×äņāüņ”Øņāü ļ░Å ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ®ņØś ļéśņØ┤ļīĆļ│ä ĒŖ╣ņä▒ņØä ļČäņäØĒĢśĻ│Āņ×É ļ│Ė ņŚ░ĻĄ¼ļź╝ ņŗ£Ē¢ēĒ¢łļŗż.
ļīĆņāüĻ│╝ ļ░®ļ▓Ģ
1. ļīĆņāü
2018ļģä 1-12ņøöņŚÉ ĒĢ£ĻĄŁ ņä£ņÜĖņØś ļŗ©ņØ╝ ņØæĻĖēņØśļŻīņä╝Ēä░ ņØæĻĖēņŗżļĪ£ ļ░®ļ¼ĖĒĢ£ 18ņäĖ ņØ┤ĒĢś ĒÖśņ×É ņżæ Ēć┤ņŗżņ¦äļŗ©ņØ┤ ņĢäļéśĒĢäļØĮņŗ£ņŖżņØĖ ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ Ē¢łļŗż. ĻĄŁņĀ£ņ¦łļ│æļČäļźś 10ĒīÉ(International Classification of Diseases, 10th revision)ņŚÉ ļö░ļźĖ ņĢäļéśĒĢäļØĮņŗ£ņŖż ņ¦äļŗ© ņĮöļō£(T50.9, T63.0, T63.1, T63.2, T63.3, T63.4, T63.5, T63.6, T63.9, T78.0, T78.2, T80.5, T88.6, Y57.9)ļĪ£ Ļ▓ĆņāēĒĢ£ ĒÖśņ×ÉņØś ņĀäņ×ÉņØśļ¼┤ĻĖ░ļĪØņØä ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒ¢łļŗż. ļ│Ė ņŚ░ĻĄ¼ļŖö ļ│ĖņøÉ ņ×äņāüņŚ░ĻĄ¼ņŗ¼ņØśņ£äņøÉĒÜīņØś ņŖ╣ņØĖņØä ņ¢╗Ļ│Ā ņŗ£Ē¢ēĒ¢łļŗż(IRB No. 2019-0771).
2. ņ¦äļŗ©ĻĖ░ņżĆ
ņāüĻĖ░ ĒÖśņ×ÉņØś ņĀäņ×ÉņØśļ¼┤ĻĖ░ļĪØņØä ĒÖĢņØĖĒĢśņŚ¼ 2006ļģä National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium[1]Ļ│╝ 2011ļģä World Allergy Organization[2]ņŚÉņä£ ļ░£Ēæ£ĒĢ£ ņ¦äļŻīņ¦Ćņ╣©ņØś ņĀĢņØśņŚÉ ņżĆĒĢśņŚ¼, ņ¦äļŗ©ņØä ĒÖĢņØĖĒ¢łļŗż. ĻĄ¼ņ▓┤ņĀüņ£╝ļĪ£, ņäĖ ĻĖ░ņżĆ ņżæ ĒĢśļéś ņØ┤ņāüņØä ņČ®ņĪ▒ĒĢśļ®┤ ņĢäļéśĒĢäļØĮņŗ£ņŖżļĪ£ ņĀĢņØśĒ¢łļŗż(Table 1).
3. ņ×ÉļŻīņłśņ¦æ
Ēæ£ņżĆĒÖöļÉ£ ņ”ØļĪĆļ│┤Ļ│Āņ¢æņŗØņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņØæĻĖēņŗż ļ░®ļ¼Ė ļŗ╣ņŗ£ ĒÖśņ×ÉņØś ņä▒ļ│ä, ļéśņØ┤, ņĢīļĀłļź┤ĻĖ░ ļ░Å ņĢäļéśĒĢäļØĮņŗ£ņŖż Ļ│╝Ļ▒░ļĀź, ņ£Āļ░£ ņČöņĀĢ ņøÉņØĖ ļ¼╝ņ¦ł, ņ”Øņāü, ņ┤łĻĖ░ ĒÖ£ļĀźņ¦ĢĒøä, ņ╣śļŻīļ░®ļ▓Ģ(ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ® ĒżĒĢ©), ņ×ģņøÉ, ņżæĒÖśņ×Éņŗż ņ×ģņøÉ, ņŗ¼ņןņĀĢņ¦Ć, ņé¼ļ¦ØņØä ņĪ░ņé¼Ē¢łļŗż. ļéśņØ┤ļīĆ ļČäļźś ĻĖ░ņżĆņØĆ ņśüņĢäĻĖ░ļŖö 1ņäĖ ļ»Ėļ¦ī, ĒĢÖļĀ╣ņĀäĻĖ░ļŖö 1-5ņäĖ, ĒĢÖļĀ╣ĻĖ░ļŖö 6-11ņäĖ, ņ▓ŁņåīļģäĻĖ░ļŖö 12-18ņäĖļĪ£ Ļ░üĻ░ü ņĀĢņØśĒ¢łļŗż.
4. ĒåĄĻ│ä
ņŚ░ņåŹĒśĢ ļ│ĆņłśļŖö ĒÅēĻĘĀ ļ░Å Ēæ£ņżĆĒÄĖņ░© ļśÉļŖö ņżæņĢÖĻ░Æ ļ░Å ņé¼ļČäņ£äņłś ļ▓öņ£äļĪ£, ļ▓öņŻ╝ĒśĢ ļ│ĆņłśļŖö ņłś ļ░Å ļ░▒ļČäņ£©ļĪ£ Ļ░üĻ░ü Ēæ£ņŗ£Ē¢łļŗż. ņ£Āļ░£ ņČöņĀĢ ņøÉņØĖ ļ¼╝ņ¦ł ļģĖņČ£ Ēøä ņ”Øņāü ļ░£ņāØĻ╣īņ¦Ć ņŗ£Ļ░äņØĆ ņĀĢĻĘ£ļČäĒżļź╝ ļ│┤ņŚ¼ Student t-testļź╝, ņ×äņāüņ”Øņāü, ņ£Āļ░£ ņČöņĀĢ ņøÉņØĖ ļ¼╝ņ¦ł, ņ╣śļŻīņØś ļéśņØ┤ļīĆļ│ä ņ░©ņØ┤ļŖö Fisher exact testļź╝ Ļ░üĻ░ü ņé¼ņÜ®Ē¢łļŗż. ļČäņäØņŚÉņä£ P < 0.05ļź╝ ĒåĄĻ│äņĀü ņ£ĀņØśņä▒ņØ┤ ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ņĀĢņØśĒ¢łļŗż. ĒåĄĻ│äņĀü ļČäņäØņŚÉļŖö SPSS ver. 21.0 (IBM Co., Armonk, NY)ņØä ņé¼ņÜ®Ē¢łļŗż.
Ļ▓░Ļ│╝
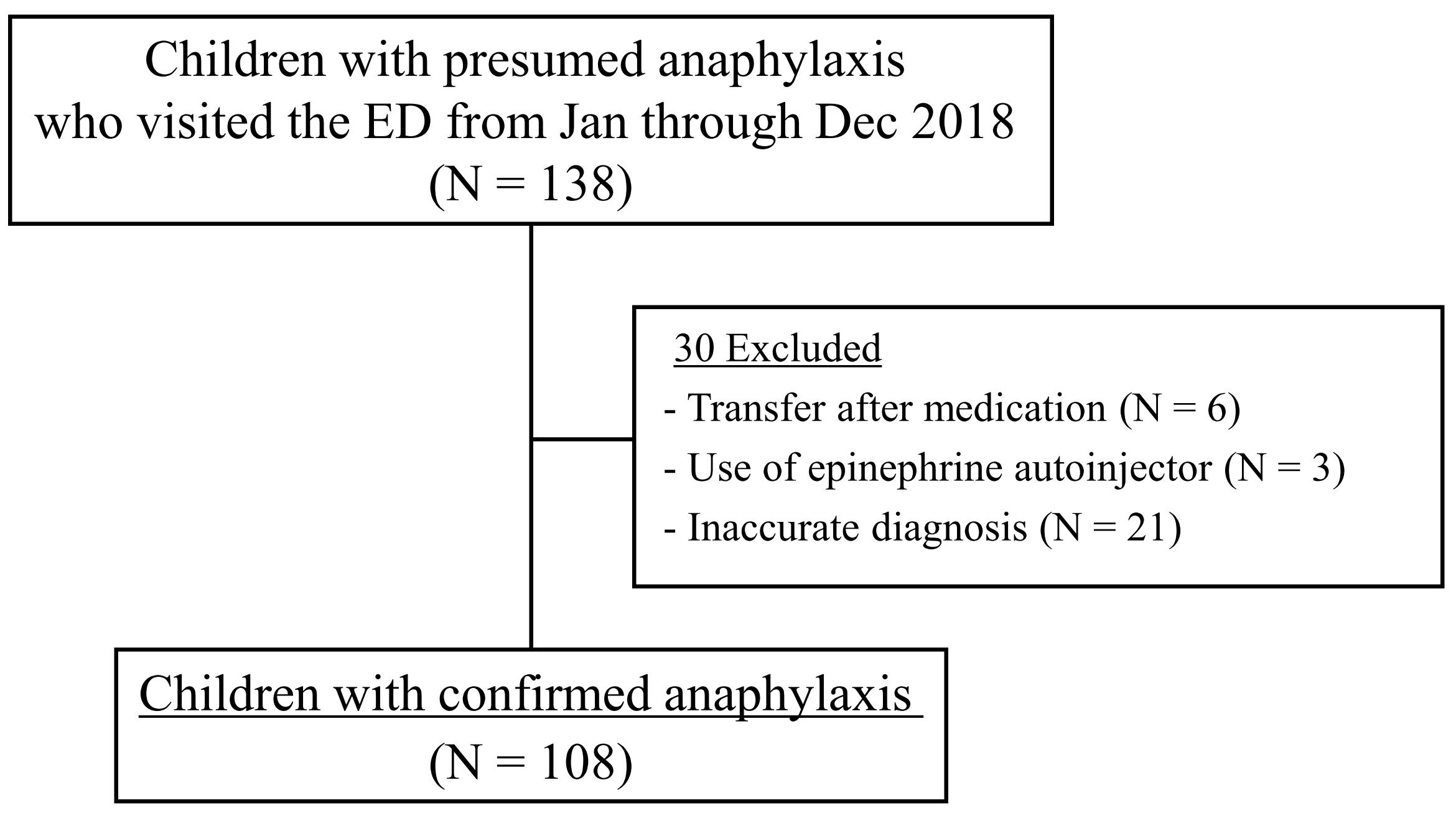
Ēć┤ņŗżņ¦äļŗ© ĻĖ░ņżĆ ņĢäļéśĒĢäļØĮņŗ£ņŖż ĒÖśņ×ÉļŖö 138ļ¬ģņ£╝ļĪ£, ņŚ░ĻĄ¼ĻĖ░Ļ░äņŚÉ ņØæĻĖēņŗżņØä ļ░®ļ¼ĖĒĢ£ ņåīņĢäņ▓Łņåīļģä ĒÖśņ×É 36,245ļ¬ģņØś 0.4%ļź╝ ņ░©ņ¦ĆĒ¢łļŗż. ņŚ¼ĻĖ░ņä£ ņ×ÉĻ░ĆņŻ╝ņé¼ņÜ® ņŚÉĒö╝ļäżĒöäļ”░ ĻĘ╝ņ£Īļé┤ņŻ╝ņé¼ Ēøä ļ░®ļ¼ĖĒĢ£ 3ļ¬ģ, ņÖĖļČĆ ļ│æņøÉņŚÉņä£ ņŚÉĒö╝ļäżĒöäļ”░ņØä ĒżĒĢ©ĒĢ£ ņĢĮ Ēł¼ņŚ¼ Ēøä ņØ┤ņåĪļÉ£ 6ļ¬ģ, ņĢäļéśĒĢäļØĮņŗ£ņŖż ņ¦äļŗ© ĻĖ░ņżĆņØä ļ¦īņĪ▒ĒĢśņ¦Ć ņĢŖļŖö 21ļ¬ģņØä ņĀ£ņÖĖĒĢ£ 108ļ¬ģņØä ņŚ░ĻĄ¼ļīĆņāüņ×ÉļĪ£ ļČäņäØĒ¢łļŗż(Fig. 1). ņāüĻĖ░ 138ļ¬ģ ņżæ ņĢĮ Ēł¼ņŚ¼ Ēøä ņØæĻĖēņŗż ļ░®ļ¼ĖĒĢ£ 9ļ¬ģņØä ņĀ£ņÖĖĒĢ£ 129ļ¬ģ ņżæ 108ļ¬ģņØ┤ ņĢäļéśĒĢäļØĮņŗ£ņŖżļĪ£ ņĄ£ņóģ ĒÖĢņØĖļÉśņ¢┤ ņĢäļŗłĒĢäļØĮņŗ£ņŖż ņ¦äļŗ©ņØś ĒŖ╣ņØ┤ļÅäļŖö 83.7%ņśĆļŗż.
ņŚ░ĻĄ¼ļīĆņāüņ×ÉņØś ļéśņØ┤ ņżæņĢÖĻ░ÆņØĆ 4ņäĖ(ņé¼ļČäņ£äņłś ļ▓öņ£ä, 2-14ņäĖ)ņśĆĻ│Ā, ļé©ņ×ÉļŖö 61ļ¬ģ(56.5%)ņØ┤ņŚłļŗż. ļéśņØ┤ļīĆļ│ä ļČäĒżļŖö ĒĢÖļĀ╣ņĀäĻĖ░Ļ░Ć 55ļ¬ģ(50.9%)ņ£╝ļĪ£ Ļ░Ćņן ĒØöĒ¢łĻ│Ā, ĻĘĖ ņÖĖ ņ▓ŁņåīļģäĻĖ░(34ļ¬ģ[31.5%]), ĒĢÖļĀ╣ĻĖ░(16ļ¬ģ[14.8%]), ņśüņĢäĻĖ░(3ļ¬ģ[2.8%]) ņł£ņØ┤ņŚłļŗż(Table 2). ņĢīļĀłļź┤ĻĖ░ ļ░Å ņĢäļéśĒĢäļØĮņŗ£ņŖż Ļ│╝Ļ▒░ļĀźņØä Ļ░Ćņ¦ä ĒÖśņ×ÉļŖö Ļ░üĻ░ü 81ļ¬ģ(75.0%) ļ░Å 7ļ¬ģ(6.5%)ņØ┤ņŚłļŗż.
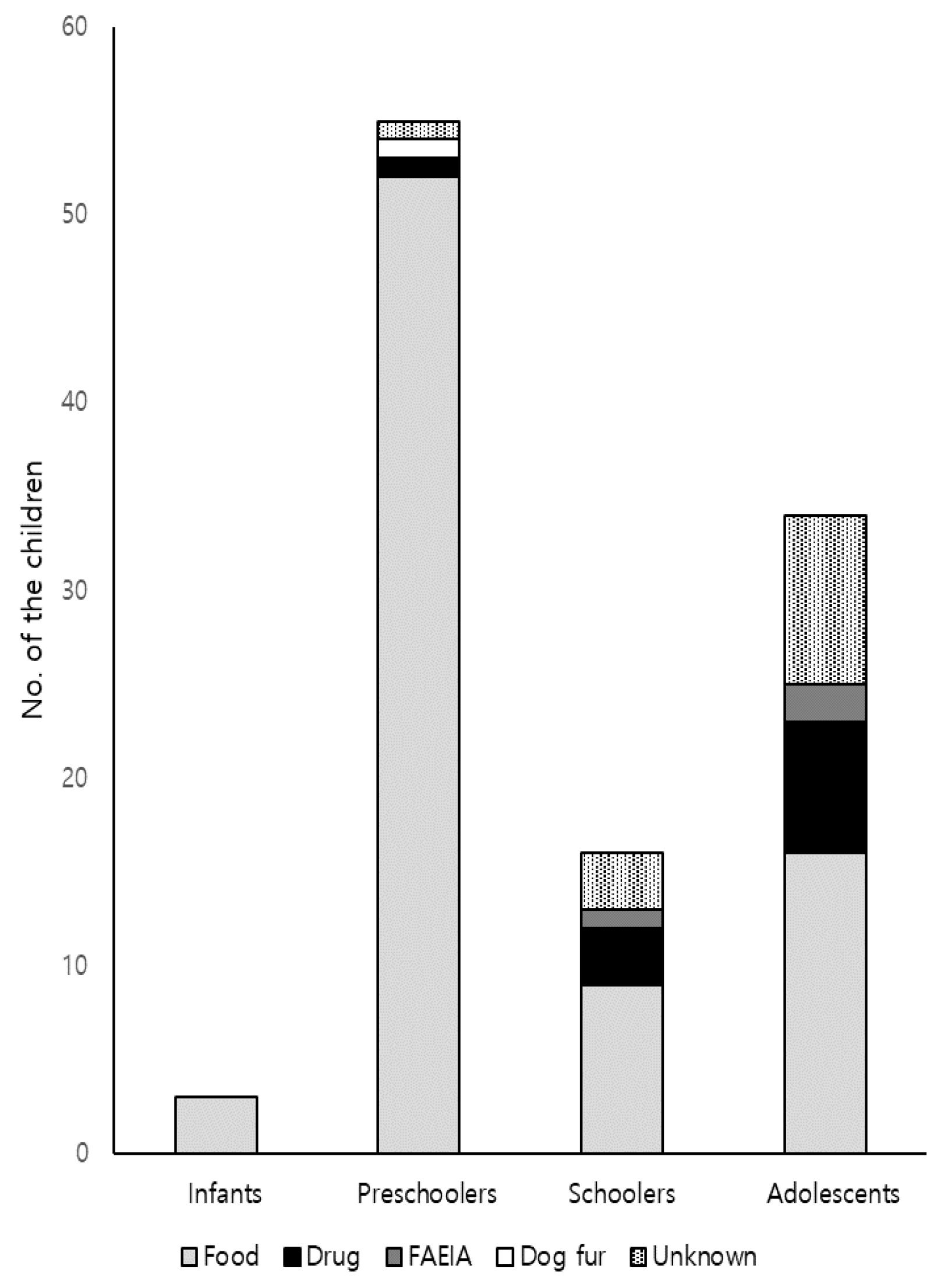
ņ£Āļ░£ ņČöņĀĢ ņøÉņØĖ ļ¼╝ņ¦łļĪ£ļŖö ņŗØĒÆłņØ┤ 80ļ¬ģ(74.1%)ņ£╝ļĪ£ Ļ░Ćņן ļ¦ÄņĢśĻ│Ā, ĻĘĖ ņÖĖ ņĢĮ 11ļ¬ģ(10.2%), ņŗØĒÆł ņŚ░Ļ┤Ć ņÜ┤ļÅÖ ņ£Āļ░£ ņĢäļéśĒĢäļØĮņŗ£ņŖż(food-associated, exercise-induced anaphylaxis, FAEIA) 3ļ¬ģ(2.8%), Ļ░ĢņĢäņ¦ĆĒäĖ 1ļ¬ģ(0.9%), ņøÉņØĖ ļ»ĖņāüņØ┤ 13ļ¬ģ(12.0%)ņØ┤ņŚłļŗż(Table 2). ļģĖņČ£ Ēøä ņ”Øņāü ļ░£ņāØĻ╣īņ¦Ć ņŗ£Ļ░äņØĆ ņØīņŗØņØ┤ 1.5 ┬▒ 1.4ņŗ£Ļ░äņØ┤ņŚłĻ│Ā ņĢĮņØĆ 1.6 ┬▒ 1.4ņŗ£Ļ░äņ£╝ļĪ£, ņØīņŗØĻ│╝ ņĢĮļ¼╝ņŚÉ ņØśĒĢ£ ļæÉ ĻĄ░ Ļ░äņŚÉ ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļŖö ņŚåņŚłļŗż. ļ¬©ļōĀ ļéśņØ┤ļīĆņŚÉņä£ ņØīņŗØņØ┤ Ļ░Ćņן ĒØöĒ¢łĻ│Ā ļéśņØ┤Ļ░Ć ņ”ØĻ░ĆĒĢĀņłśļĪØ ņĢĮ ļ░Å ņøÉņØĖ ļ»ĖņāüņØś ļ╣łļÅäĻ░Ć ļŖśņ¢┤ļé¼ļŗż(Fig. 2). ĒĢśņ¦Ćļ¦ī ņśüņĢäĻĖ░ ĒÖśņ×É 3ļ¬ģ ļ¬©ļæÉ ņØīņŗØ ļģĖņČ£ Ēøä ļ░£ņāØĒ¢łĻ│Ā, ĒĢÖļĀ╣ņĀäĻĖ░ ĒÖśņ×É ņżæ ņØīņŗØ 52ļ¬ģ(94.5%), ņĢĮ, Ļ░ĢņĢäņ¦ĆĒäĖ, ņøÉņØĖ ļ»ĖņāüņØ┤ Ļ░ü 1ļ¬ģ(1.8%)ņØ┤ņŚłļŗż. ĻĖ░ĒāĆ ļéśņØ┤ļīĆ ĒÖśņ×ÉņŚÉņä£ļÅä ņØīņŗØņØ┤ Ļ░Ćņן ĒØöĒ¢łņ¦Ćļ¦ī, ĒĢÖļĀ╣ĻĖ░ 9ļ¬ģ(56.3%), ņ▓ŁņåīļģäĻĖ░ 16ļ¬ģ(47.1%)ņ£╝ļĪ£ ļéśņØ┤Ļ░Ć ņ”ØĻ░ĆĒĢśļ®┤ņä£ ĻĘĖ ļ╣łļÅäļŖö ņĀÉņ░© Ļ░ÉņåīĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņśĆļŗż.
ņ×äņāüņ”ØņāüņØĆ Ēö╝ļČĆņ”ØņāüņØ┤ Ļ░Ćņן ĒØöĒ¢łĻ│Ā(105ļ¬ģ[97.2%]), ĒśĖĒØĪĻ│ä ņ”Øņāü 97ļ¬ģ(89.8%), ņ£äņןĻ┤Ć ņ”Øņāü 31ļ¬ģ(28.7%), ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”Øņāü 11ļ¬ģ(10.2%) ņł£ņØ┤ņŚłļŗż(Table 3). ļéśņØ┤ļīĆļ│äļĪ£ ļ¬©ļōĀ ĒĢÖļĀ╣ņĀäĻĖ░ ĒÖśņ×ÉņŚÉņä£ Ēö╝ļČĆņ”ØņāüņØä ļ│┤ņśĆĻ│Ā, ļ¬©ļōĀ ĒĢÖļĀ╣ĻĖ░ ĒÖśņ×ÉņŚÉņä£ ĒśĖĒØĪĻ│ä ņ”ØņāüņØä ļ│┤ņśĆļŗż. ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØĆ ņ▓ŁņåīļģäĻĖ░ņŚÉņä£ Ļ░Ćņן ĒØöĒ¢łĻ│Ā, ņ£ĀņØ╝ĒĢśĻ▓ī ņ£ĀņØśĒĢ£ ļéśņØ┤ļīĆļ│ä ņ░©ņØ┤Ļ░Ć ņ׳ņŚłļŗż(P = 0.002).
ņĢäļéśĒĢäļØĮņŗ£ņŖżņØś ņ╣śļŻīļŖö ĒĢŁĒ׳ņŖżĒāĆļ»╝ņĀ£ļź╝ Ļ░Ćņן ņ×ÉņŻ╝ Ēł¼ņŚ¼Ē¢łĻ│Ā(105ļ¬ģ[97.2%]), ĒŖ╣Ē׳ Ēö╝ļČĆņ”ØņāüņØ┤ ļéśĒāĆļé£ ļ¬©ļōĀ ĒÖśņ×ÉņŚÉĻ▓ī Ēł¼ņŚ¼Ē¢łļŗż. ņŚÉĒö╝ļäżĒöäļ”░ ĻĘ╝ņ£Īļé┤ņŻ╝ņé¼ļŖö 82ļ¬ģ(75.9%)ņŚÉĻ▓ī Ēł¼ņŚ¼Ē¢łņ£╝ļ®░, ļéśņØ┤ņÖĆ ĒĢ©Ļ╗ś ņ”ØĻ░ĆĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņśĆņ£╝ļ®░, ņØ┤ļŖö ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļź╝ ļ│┤ņśĆļŗż(P = 0.037) (Table 4). ņĀĢļ¦źļé┤ ņłśņĢĪņÜöļ▓ĢļÅä ņØ┤ņÖĆ ļ╣äņŖĘĒĢ£ Ļ▓ĮĒ¢źņØä ļ│┤ņśĆļŗż. ĒĢŁĒ׳ņŖżĒāĆļ»╝ņØä Ēł¼ņŚ¼ĒĢśņ¦Ć ņĢŖņØĆ 3ļ¬ģ ļ¬©ļæÉ Ēö╝ļČĆņ”ØņāüņØä ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśĻ│Ā, ņŖżĒģīļĪ£ņØ┤ļō£ļź╝ Ēł¼ņŚ¼ĒĢśņ¦Ć ņĢŖņØĆ 15ļ¬ģ ņżæ 12ļ¬ģņØĆ ĒśĖĒØĪĻ│ä ņ”ØņāüņØä ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż. ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØä ļ│┤ņØĖ 11ļ¬ģ ļ¬©ļæÉņŚÉĻ▓ī ņŚÉĒö╝ļäżĒöäļ”░ņØä Ēł¼ņŚ¼Ē¢łļŗż. ņŚÉĒö╝ļäżĒöäļ”░ņØä Ēł¼ņŚ¼ĒĢ£ 82ļ¬ģ ņżæ ĒśĖĒØĪĻ│ä ņ”ØņāüņØĆ 73ļ¬ģņŚÉņä£, ņ£äņןĻ┤Ć ņ”ØņāüņØĆ 25ļ¬ģņŚÉņä£, Ļ░üĻ░ü ļ│┤ņśĆļŗż. ņŚÉĒö╝ļäżĒöäļ”░ņØä Ēł¼ņŚ¼ĒĢśņ¦Ć ņĢŖņØĆ 26ļ¬ģ ļ¬©ļæÉ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØä ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśĻ│Ā, ņØ┤ ņżæ 17ļ¬ģņØĆ ĒśĖĒØĪĻ│żļ×ĆņØä ĒśĖņåīĒ¢łņ¦Ćļ¦ī ņé░ņåīĒżĒÖöļÅä Ļ░Éņåī, ņīĢņīĢĻ▒░ļ”╝ ļśÉļŖö Ēśæņ░®ņØīņØä ļÅÖļ░śĒĢśņ¦Ć ņĢŖņĢśĻ│Ā, ļéśļ©Ėņ¦Ć 9ļ¬ģņØĆ ļ│ĄĒåĄņØĆ ņ׳ņ¦Ćļ¦ī ĻĄ¼ņŚŁ, ĻĄ¼ĒåĀ, ņäżņé¼ ļō▒ņØä ļÅÖļ░śĒĢśņ¦Ć ņĢŖņĢśļŗż.
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņ×ģņøÉ ĒÖśņ×ÉļŖö 4ļ¬ģ(3.7%)ņØ┤ņŚłĻ│Ā, ļ¬©ļæÉ ņĪ░ĻĖ░ņŚÉ ņŚÉĒö╝ļäżĒöäļ”░ņØä Ēł¼ņŚ¼Ē¢łņ¦Ćļ¦ī ņ”ØņāüņØ┤ ņ¦ĆņåŹĒĢśņŚ¼ ņ×ģņøÉ ņ╣śļŻīļź╝ ļ░øņĢśļŗż. ņØ┤ 4ļ¬ģņØś ņ£Āļ░£ ņČöņĀĢ ņøÉņØĖ ļ¼╝ņ¦łņØĆ ļĢģņĮ®, ļ®öļ░Ć, ņāłņÜ░, ĒĢŁņāØņĀ£Ļ░Ć Ļ░ü 1ļ¬ģņØ┤ņŚłĻ│Ā, ļ¬©ļæÉ ĒĢ®ļ│æņ”Ø ņŚåņØ┤ Ēć┤ņøÉĒ¢łļŗż. ņżæĒÖśņ×Éņŗż ņ×ģņøÉ ļ░Å ņé¼ļ¦ØņØĆ ņŚåņŚłļŗż.
Ļ│Āņ░░
ļ│Ė ņŚ░ĻĄ¼ļŖö ņśüņĢäĻĖ░ ļ░Å ĒĢÖļĀ╣ņĀäĻĖ░ ņĢäļéśĒĢäļØĮņŗ£ņŖż ĒÖśņ×ÉņŚÉņä£ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”Øņāü ļ░Å ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ® ļ╣łļÅäĻ░Ć ņ▓ŁņåīļģäĻĖ░ļ│┤ļŗż ļé«ņØīņØä ļ│┤ņŚ¼ņżĆļŗż. ņĀäņ×ÉņØś ĒÖśņ×ÉĻĄ░ņØĆ ĻĖ░ļÅäĒÅÉņćä ļ░Å ĒśĖĒØĪĻ│żļ×ĆņŚÉ ļīĆĒĢ£ ņāØļ”¼ņĀü ļ│┤ņāüļŖźļĀźņØ┤ ļ¢©ņ¢┤ņ¦ĆļŖö ļ░śļ®┤, ĒśłņĢĢ ņĀĆĒĢśņŚÉ ļīĆĒĢ£ ņ╣┤ĒģīņĮ£ņĢäļ»╝ ļČäļ╣äļź╝ ĒåĄĒĢ£ ļ│┤ņāüļŖźļĀźņØ┤ ņÜ░ņłśĒĢśņŚ¼ ņć╝Ēü¼Ļ░Ć ļŖ”Ļ▓ī ļ░£Ļ▓¼ļÉśĻĖ░ ņēĮļŗż[11]. ņŚÉĒö╝ļäżĒöäļ”░ņØä ļŖ”Ļ▓ī Ēł¼ņŚ¼ĒĢśļ®┤ ņĢäļéśĒĢäļØĮņŗ£ņŖż ņ¦ĆņŚ░ ļ░śņØæņØ┤ ļŹö ĒØöĒĢśĻ│Ā ņŗ¼ĒĢśĻ▓ī ņØ╝ņ¢┤ļé£ļŗż[12]. ļśÉĒĢ£, ņ¦äļŻīņ¦Ćņ╣©ņØĆ ņśüņĢäĻĖ░ ļ░Å ĒĢÖļĀ╣ņĀäĻĖ░ ĒÖśņ×ÉņŚÉņä£ ņŻ╝ļÉ£ ņ£Āļ░£ ņČöņĀĢ ņøÉņØĖ ļ¼╝ņ¦łņØĖ ņØīņŗØņŚÉ ļģĖņČ£ Ēøä ĻĖēņä▒ ĒśĖĒØĪĻ│żļ×Ć ļ░Å ņĀÉļ¦ēĒö╝ļČĆņ”ØņāüņØ┤ ļ░£ņāØĒĢśļ®┤ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØ┤ ņŚåņØ┤ļÅä ņĢäļéśĒĢäļØĮņŗ£ņŖżļĪ£ Ļ░äņŻ╝ĒĢśĻ│Ā ņŚÉĒö╝ļäżĒöäļ”░ņØä ņĀüĻĘ╣ņĀüņ£╝ļĪ£ Ēł¼ņŚ¼ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż[13,14].
ņ”ØņāüņØä ļéśņØ┤ļīĆļ│äļĪ£ ĻĄ¼ļČäĒĢśņŚ¼ ĻĖ░ņłĀĒĢ£ ņØ┤ņĀä ņŚ░ĻĄ¼Ļ░Ć ļČĆņĪ▒ĒĢśņŚ¼ ļ╣äĻĄÉĒĢśĻĖ░ ņ¢┤ļĀĄņ¦Ćļ¦ī, ļ¬©ļōĀ ļéśņØ┤ļīĆņŚÉņä£ Ēö╝ļČĆņ”ØņāüņØ┤ Ļ░Ćņן ĒØöĒ¢łļŹś ņĀÉņØĆ ņØ┤ņĀä ņŚ░ĻĄ¼ņÖĆ ņØ╝ņ╣śĒĢ£ļŗż[7-10]. ņåīņĢä ļ░Å ņä▒ņØĖņØś ņ”ØņāüņØä ļ╣äĻĄÉĒĢ£ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØ┤ ņä▒ņØĖņŚÉņä£ ņ£ĀņØśĒĢśĻ▓ī ļŹö ĒØöĒ¢łĻ│Ā, ņ£äņןĻ┤Ć ņ”ØņāüņØĆ ņåīņĢäņŚÉņä£ ĒØöĒĢ£ Ļ▓ĮĒ¢źņØä ļ│┤ņśĆņ¦Ćļ¦ī ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļŖö ņŚåņŚłļŗż[9]. ņØ┤ļŖö ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØ┤ ņ▓ŁņåīļģäĻĖ░ņŚÉņä£ Ļ░Ćņן ĒØöĒ¢łļŹś ņĀÉ ļ░Å ļéśņØ┤ ņ”ØĻ░ĆņŚÉ ļö░ļØ╝ ņ£äņןĻ┤Ć ņ”ØņāüņØ┤ Ļ░ÉņåīĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņØĖ ņĀÉĻ│╝ ņØ╝ņ╣śĒĢ£ļŗż. ņ£Āļ░£ ņøÉņØĖņØĆ ļ¬©ļōĀ ļéśņØ┤ļīĆņŚÉņä£ ņØīņŗØņØ┤ Ļ░Ćņן ĒØöĒĢ£ ņ£Āļ░£ ņČöņĀĢ ņøÉņØĖ ļ¼╝ņ¦łņØ┤ņŚłĻ│Ā ņä▒ņØĖņŚÉņä£ ņāüļīĆņĀüņ£╝ļĪ£ ņĢĮņØś ļ╣łļÅäĻ░Ć ņ”ØĻ░ĆĒ¢łļŖöļŹ░[8,9], ņØ┤ļŖö ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ļéśņØ┤ ņ”ØĻ░ĆņŚÉ ļö░ļØ╝ ņØīņŗØ ļ╣łļÅäļŖö Ļ░ÉņåīĒĢśĻ│Ā(P = 0.001) ņĢĮņØś ļ╣łļÅäļŖö ņ”ØĻ░Ć(P = 0.011)ĒĢ£ ņĀÉĻ│╝ ņØ╝ņ╣śĒĢ£ļŗż.
ņĢäļéśĒĢäļØĮņŗ£ņŖż ļ░£ņāØļźĀņØĆ ņ”ØĻ░ĆĒĢśļŖö ņČöņäĖļĪ£, ĒĢ£ĻĄŁ Ļ▒┤Ļ░Ģļ│┤ĒŚśņŗ¼ņé¼ĒÅēĻ░ĆņøÉ ņ×ÉļŻīļź╝ ļČäņäØĒĢ£ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, ņĢäļéśĒĢäļØĮņŗ£ņŖż ĒÖśņ×ÉĻ░Ć 2010ļģäņØś 0.02%ņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ 2014ļģäņŚÉļŖö 0.04%ļĪ£ ņ”ØĻ░ĆĒ¢łļŗż[15]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņØæĻĖēņŗż ĒÖśņ×É ņżæ 0.3%Ļ░Ć Ēć┤ņøÉ ņŗ£ ņĢäļéśĒĢäļØĮņŗ£ņŖżļĪ£ ņ¦äļŗ©ļÉÉļŗż. ļö░ļØ╝ņä£ ņĪ░ĻĖ░ ņ¦äļŗ© ļ░Å ņŚÉĒö╝ļäżĒöäļ”░ Ēł¼ņŚ¼Ļ░Ć ņżæņÜöĒĢ£ļŹ░, ņ¦äļŗ© ļ░Å ņ╣śļŻīĻ░Ć ļŖ”ņ¢┤ņ¦Ćļ®┤ ņ×ģņøÉ ļ╣łļÅäĻ░Ć ņ”ØĻ░ĆĒĢśĻ│Ā ļō£ļ¼╝Ļ▓ī ņé¼ļ¦ØņØä ņ┤łļלĒĢĀ ņłś ņ׳ļŗż[5,6]. ņśüĻĄŁņŚÉņä£ 10ļģäĻ░ä 202ļ¬ģņØ┤[16], ĒśĖņŻ╝ņŚÉņä£ļŖö 9ļģäĻ░ä 112ļ¬ģ[17]ņØ┤ Ļ░üĻ░ü ņé¼ļ¦ØĒ¢łļŗżĻ│Ā ļ│┤Ļ│ĀĒ¢łņ£╝ļ®░, ĒĢ£ĻĄŁņŚÉņä£ļÅä 2001-2004ļģäņŚÉ 5ļ¬ģņØ┤ ņé¼ļ¦ØĒ¢łļŗżĻ│Ā ļ│┤Ļ│ĀĒ¢łļŗż[18]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņé¼ļ¦Ø ĒÖśņ×ÉļŖö ņŚåņŚłņ¦Ćļ¦ī, ņ×ģņøÉ ĒÖśņ×ÉļŖö 4ļ¬ģņØ┤ņŚłļŗż. ĒĢ£ĻĄŁņØś ņĀäņ▓┤ ļéśņØ┤ ĒÖśņ×É ļīĆņāü ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņ×ģņøÉņØĆ 91ļ¬ģ ņżæ 6ļ¬ģņØ┤ņŚłĻ│Ā ņżæĒÖśņ×Éņŗż ņ×ģņøÉ ļ░Å ņé¼ļ¦ØņØĆ ņŚåņŚłņ£╝ļ®░[9], ņśüĻĄŁ ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņĢäļéśĒĢäļØĮņŗ£ņŖż ļ░£ņāØ ļ░Å ņ×ģņøÉņØĆ ņ”ØĻ░ĆĒĢśņ¦Ćļ¦ī, ņé¼ļ¦ØņŚÉļŖö Ēü░ ņ░©ņØ┤Ļ░Ć ņŚåļŗżĻ│Ā ļ│┤Ļ│ĀĒ¢łļŗż[19].
ņŚÉĒö╝ļäżĒöäļ”░ ņĪ░ĻĖ░ ņé¼ņÜ®ņ£╝ļĪ£ ņé¼ļ¦ØĻ│╝ Ļ░ÖņØĆ ņŗ¼Ļ░üĒĢ£ ņśłĒøäļź╝ ņśłļ░®ĒĢĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£ ņżæņÜöĒĢśļŗż[5,6,20]. ņŚÉĒö╝ļäżĒöäļ”░ņØ┤ ņØ╝ņ░© ņäĀĒāØ ņĢĮņĀ£ņØ┤ņ¦Ćļ¦ī ņØśļŻīņ¦äņØ┤ ņ”ØņāüņØä Ļ░äĻ│╝ĒĢśĻ▒░ļéś ļČĆņ×æņÜ®ņØä ņÜ░ļĀżĒĢśņŚ¼ ņŚÉĒö╝ļäżĒöäļ”░ Ēł¼ņŚ¼ļź╝ ņŻ╝ņĀĆĒĢśĻĖ░ļÅä ĒĢ£ļŗż[21,22]. ņĢäļéśĒĢäļØĮņŗ£ņŖż ņ¦äļŗ©ņØĆ ņ”ØĻ░ĆĒĢśņ¦Ćļ¦ī ņé¼ļ¦ØņØĆ ļō£ļ¼╝ņ¢┤ ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ®ņØ┤ ņĀüņØĆ Ļ▓ĮĒ¢źņØä ļ│┤ņØ┤Ļ│Ā[23], ņŗżņĀ£ļĪ£ ņé¼ņÜ® ļ╣łļÅäņØś ļéśņØ┤ļīĆ ļ░Å ņ¦ĆņŚŁ ļ│ä ĒÄĖņ░©Ļ░Ć ņŗ¼ĒĢśļŗż[4,24-26]. ĒĢ£ĻĄŁņŚÉņä£ 5ļģäĻ░ä ņĀäņ▓┤ ļéśņØ┤ ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ Ļ▒┤Ļ░Ģļ│┤ĒŚśņŗ¼ņé¼ĒÅēĻ░ĆņøÉ ņ×ÉļŻī ļČäņäØ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, ņŚÉĒö╝ļäżĒöäļ”░ņØ┤ ņĀäņ▓┤ ĒÖśņ×ÉņØś 35.8%ņŚÉņä£ ņé¼ņÜ®ļÉÉļŗż[4]. ļ»ĖĻĄŁņŚÉņä£ļŖö 1ļģäĻ░ä ņØæĻĖēņŗżņØä ļ░®ļ¼ĖĒĢ£ ņĢäļéśĒĢäļØĮņŗ£ņŖż ņåīņĢäĒÖśņ×ÉņØś 48%ņŚÉņä£[24], ņŗ▒Ļ░ĆĒżļź┤ņŚÉņä£ļŖö ņØæĻĖēņŗżņØä ļ░®ļ¼ĖĒĢ£ ņĢäļéśĒĢäļØĮņŗ£ņŖż ņåīņĢäĒÖśņ×ÉņØś 86.6%ņŚÉņä£ Ļ░üĻ░ü ņé¼ņÜ®ļÉÉļŗż[25]. ĻĘĖļ”¼Ļ│Ā ņåīņĢä ĒÖśņ×ÉļŖö ņä▒ņØĖļ│┤ļŗż ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ® ļ╣łļÅäĻ░Ć ļé«ļŗżļŖö ļ│┤Ļ│ĀļÅä ņ׳ļŗż[26]. ĒĢŁĒ׳ņŖżĒāĆļ»╝ņĀ£ ļ░Å ņŖżĒģīļĪ£ņØ┤ļō£Ļ░Ć ņŚÉĒö╝ļäżĒöäļ”░ņØä ļīĆņ▓┤ĒĢĀ ņłś ņŚåņ£╝ļ»ĆļĪ£, ņØæĻĖēņŗż ņØśļŻīņ¦äņŚÉĻ▓ī ņ¦äļŻīņ¦Ćņ╣©ņŚÉ ļö░ļØ╝ ņ¦äļŻīĒĢśļÅäļĪØ ĻĄÉņ£ĪĒĢ©ņ£╝ļĪ£ņŹ© ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ® ļ╣łļÅäļź╝ ņĀ£Ļ│ĀĒĢĀ ņłś ņ׳ļŗż[19,27,28]. ļśÉĒĢ£, ņŚÉĒö╝ļäżĒöäļ”░ ĻĘ╝ņ£Īļé┤ņŻ╝ņé¼ļŖö ļČĆņ×æņÜ®ņØ┤ ļō£ļ¼╝ņ¢┤, ļŹö ņĀüĻĘ╣ņĀüņ£╝ļĪ£ ņé¼ņÜ®ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż[2,20,21]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņŚÉĒö╝ļäżĒöäļ”░ņØ┤ ņĀäņ▓┤ ņŚ░ĻĄ¼ļīĆņāüņ×ÉņØś 75.9%ņŚÉņä£ ņé¼ņÜ®ļÉśņ¢┤ ņØ┤ņĀä ļ│┤Ļ│Āļ│┤ļŗż ļ╣äĻĄÉņĀü ļåÆņĢśļŗż. Ē¢źĒøä ņĀĢĻĖ░ņĀüņØĖ ņ¦äļŻīņ¦Ćņ╣© ĻĄÉņ£Ī ļ░Å ņ×äņāüņ¦äļŻīņ▓┤Ļ│ä(clinical pathway) ĻĄ¼ņČĢņØä ĒåĄĒĢ┤, ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ®ņØä ļŖśļ”┤ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż.
ņŚÉĒö╝ļäżĒöäļ”░ ļ░Å ņĀĢļ¦źļé┤ ņłśņĢĪņÜöļ▓Ģ ņé¼ņÜ®ņØ┤ ļéśņØ┤ ņ”ØĻ░ĆņŚÉ ļö░ļØ╝ ņ£ĀņØśĒĢśĻ▓ī ņ”ØĻ░ĆĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņØĖ Ļ▓āņØĆ ņ▓ŁņåīļģäĻĖ░ ĒÖśņ×ÉņŚÉņä£ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØ┤ ĒØöĒĢ£ Ļ▓āĻ│╝ ņŚ░Ļ┤ĆļÉ£ Ļ▓āņ£╝ļĪ£ ņČöņĀĢĒĢĀ ņłś ņ׳ļŗż. ņĢäļéśĒĢäļØĮņŗ£ņŖż ņ╣śļŻīņØś ļéśņØ┤ļīĆļ│ä ņ░©ņØ┤ņŚÉ Ļ┤ĆĒĢ£ ņŚ░ĻĄ¼ļŖö ļČĆņĪ▒ĒĢ£ ņŗżņĀĢņØ┤ļŗż. ļö░ļØ╝ņä£, ņןĻĖ░Ļ░ä ļīĆĻĘ£ļ¬© ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ ņ¢┤ļ”░ ņåīņĢäņŚÉņä£ ļé«ņØĆ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”Øņāü ļ░Å ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ® ļ╣łļÅäņØś ņŚ░Ļ┤ĆņØä ņ×ģņ”ØĒĢĀ ĒĢäņÜöĻ░Ć ņ׳ļŗż.
ļ│Ė ņŚ░ĻĄ¼ņØś ņĀ£ĒĢ£ņĀÉņ£╝ļĪ£ļŖö ļŗ©ņØ╝ ĻĖ░Ļ┤Ć ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ņØĖ ņĀÉĻ│╝ ļ╣äĻĄÉņĀü ņ¦¦ņØĆ ņŚ░ĻĄ¼ĻĖ░Ļ░ä ļĢīļ¼ĖņŚÉ ņŚ░ĻĄ¼ļīĆņāüņ×ÉĻ░Ć ļ╣äĻĄÉņĀü ņĀüņŚłļŹś ņĀÉņØä ļōż ņłś ņ׳ļŗż. ļśÉĒĢ£, Ēć┤ņŗż ĒĢ£ņĀĢĒĢśņŚ¼, ļŗżļźĖ ņĢīļĀłļź┤ĻĖ░ Ļ┤ĆļĀ© ņ¦äļŗ©ņ£╝ļĪ£ ņלļ¬╗ ņ¦äļŗ©ļÉ£ ņĢäļéśĒĢäļØĮņŗ£ņŖż ĒÖśņ×Éļź╝ ĒżĒĢ©ĒĢśņ¦Ć ļ¬╗Ē¢łļŗż. Ē¢źĒøä ļŗżļźĖ ņĢīļĀłļź┤ĻĖ░ Ļ┤ĆļĀ© ņ¦äļŗ©ļ¬ģņ£╝ļĪ£ ĒżĒĢ©ĻĖ░ņżĆņØä ĒÖĢļīĆĒĢśņŚ¼ ņĢäļéśĒĢäļØĮņŗ£ņŖż ņ£äņØīņä▒ ĒÖśņ×Éļź╝ ĒżĒĢ©ĒĢśņŚ¼ ņןĻĖ░Ļ░ä ņŚ░ĻĄ¼ļź╝ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļŗż.
ņÜöņĢĮĒĢśļ®┤, ņĢäļéśĒĢäļØĮņŗ£ņŖż ĒÖśņ×É ņżæ ņśüņĢäĻĖ░ ļ░Å ĒĢÖļĀ╣ņĀäĻĖ░ ĒÖśņ×ÉļŖö ņ▓ŁņåīļģäĻĖ░ ĒÖśņ×Éļ│┤ļŗż ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”Øņāü ļ░Å ņŚÉĒö╝ļäżĒöäļ”░ ņé¼ņÜ® ļ╣łļÅäĻ░Ć ļé«ņĢśļŗż. ņĀäņ×ÉņØś ĒÖśņ×ÉĻĄ░ņŚÉņä£ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ”ØņāüņØ┤ ņŚåļŹöļØ╝ļÅä ņĢäļéśĒĢäļØĮņŗ£ņŖżļĪ£ ņØĖņ¦ĆĒĢśņŚ¼ ņ¦äļŻīņ¦Ćņ╣©ņŚÉ ļö░ļØ╝ ņĀüĻĘ╣ņĀüņ£╝ļĪ£ ņŚÉĒö╝ļäżĒöäļ”░ņØä ņé¼ņÜ®ĒĢ┤ņĢ╝ ĒĢ£ļŗż.